40 Facts You Need to Know: The Real Story of “Covid” (3)
Read the second part of the article
Part VI: Masks
Masks don’t work
At least a dozen scientific studies have shown that masks do nothing to stop the spread of respiratory viruses.

One meta-analysis published by the CDC in May 2020 found “no significant reduction in influenza transmission with the use of face masks”.
A Canadian review from July 2020 found “limited evidence that the use of masks might reduce the risk of viral respiratory infections”.
Another study with over 8000 subjects found masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection.”
There are literally too many to quote them all, but you can read a summary here.
While some studies have been done claiming to show mask do work for covid, they are all seriously flawed. One relied on self-reported surveys as data. Another was so badly designed that a panel of experts demanded it be withdrawn. A third was withdrawn after its predictions proved entirely incorrect.
The WHO commissioned its own meta-analysis in the Lancet, but that study looked only at N95 masks and only in hospitals. [For a full rundown on the bad data in this study read here.]
Aside from scientific evidence, there’s plenty of real-world evidence that masks do nothing to halt the spread of disease.
For example, North Dakota and South Dakota had near-identical “case” figures, despite one having a mask mandate and the other not:
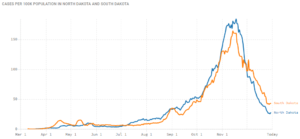
In Kansas, counties without mask mandates actually had fewer covid cases than counties with mask mandates. And despite masks being very common in Japan, they had their worst flu outbreak in decades in 2019.
Not only do masks not work, but it was widely known they did not work before 2020. A 2016 literature review published in the Journal of Oral Health found:
“There are no convincing scientific data that support the effectiveness of masks for respiratory protection.”
(This study was quietly removed from the journal’s website in June 2020, because it was “no longer relevant in the current climate”.)
Another study, published in 2020 but carried out in 2019, found “no significant effect of face masks on transmission of laboratory-confirmed influenza.”
In his 2020 review, Masks Don’t Work, Dr. Denis Rancourt cites studies from 2009, 2010, 2012, 2016, 2017 and 2019, none of which found any significant benefit at all from wearing a mask.
And, most tellingly, in their own report on influenza from 2019, the WHO itself noted that “there is no evidence that [masks are] effective in reducing transmission”.
Masks are bad for your health
Wearing a mask for long periods, wearing the same mask more than once, and other aspects of cloth masks can be bad for your health. A long study on the detrimental effects of mask-wearing was recently published by the International Journal of Environmental Research and Public Health.
Dr. James Meehan reported in August 2020 he was seeing increases in bacterial pneumonia, fungal infections, and facial rashes.
Masks are also known to contain plastic microfibers, which damage the lungs when inhaled and may be potentially carcinogenic.
Children wearing masks encourages mouth-breathing, which results in facial deformities.
People around the world have passed out due to CO2 poisoning while wearing their masks, and some children in China even suffered sudden cardiac arrest.
Moreover, masks may actually increase the likelihood of respiratory disease, a trial of cloth masks from 2015 found that: “Moisture retention, reuse of cloth masks and poor filtration may result in an increased risk of infection.”
While a study published in July 2022 found that masks, especially those worn more than once, were breeding grounds for both bacteria and fungal microbes.
Another peer-reviewed paper on mask effectiveness, from April 2022, found:
“While no cause-effect conclusions could be inferred from this observational analysis, the lack of negative correlations between mask usage and covid-19 cases and deaths suggest that the widespread use of masks was not able to reduce covid-19 transmission. Moreover, the moderate positive correlation between mask usage and deaths in Western Europe also suggests that the universal use of masks may have had harmful unintended consequences.”
Masks are bad for the planet
Millions upon millions of disposable masks have been used per month for over a year. A report from the UN found the covid-19 pandemic will likely result in plastic waste more than doubling in the next few years, and the vast majority of that is face masks.
The report goes on to warn these masks (and other medical waste) will clog sewage and irrigation systems, which will have knock-on effects on public health, irrigation and agriculture.
A study from the University of Swansea found “heavy metals and plastic fibres were released when throw-away masks were submerged in water.” These materials are toxic to both people and wildlife.
Another study, published in 2022, found that “disposable face masks and plastic gloves could pose an ongoing risk to wildlife for tens if not hundreds of years.”
Part VII: Vaccines
Covid “vaccines” are totally unprecedented
Before 2020 no successful vaccine against a human coronavirus had ever been developed. Following the advent of “covid”, we allegedly made over 20 of them in 18 months.

Scientists have been trying to develop a SARS and MERS vaccine for years with little success. Some of the failed SARS vaccines actually caused hypersensitivity to the SARS virus. Meaning that vaccinated mice could potentially get the disease more severely than unvaccinated mice. Another attempt caused liver damage in ferrets.
Whereas the theory behind traditional vaccines is that exposing the body to a weakened strain of a microorganism will trigger an immune response, many of these new covid “vaccines” are mRNA vaccines.
The mRNA (messenger ribonucleic acid) vaccines theoretically work by injecting viral mRNA into the body, where it replicates inside your cells and encourages your body to recognise, and make antigens for, the “spike proteins” of the virus.
The mRNA vaccines have been the subject of research since the 1990s, but before 2020 no mRNA vaccine was ever approved for use on humans.
Yet, following the advent of covid, two different companies made two supposedly “safe and effective” mRNA vaccines within weeks of each other.
“Covid vaccines” do not confer immunity or prevent transmission
It is readily admitted that covid “vaccines” do not confer immunity from infection and do not prevent you from passing the disease onto others. Indeed, an article in the British Medical Journal highlighted that the vaccine trials were not designed to even try and assess if the “vaccines” limited transmission.
The vaccine manufacturers themselves, upon releasing the untested mRNA gene therapies, were quite clear their product’s “efficacy” was based on “reducing the severity of symptoms”.
In October 2022 Pfizer executive Janine Small, testifying in front of the EU parliament, admitted that Pfizer never even tested if their vaccine prevented transmission of “covid” prior to its release to the public.
The vaccines were rushed and have unknown long-term effects
Vaccine development is a slow, laborious process. Usually, from development through testing and finally being approved for public use takes many years. The various vaccines for covid were all developed and approved in less than a year.
Moderna’s own website admits “it normally takes 10-15 years to develop a vaccine”, but boasts of producing their SpikeVax “within 2 months”.
Obviously, there can be no long-term safety data on chemicals that are less than a year old.
Pfizer even admits this is true in the leaked supply contract between the pharmaceutical giant, and the government of Albania: “The long-term effects and efficacy of the vaccine are not currently known and that there may be adverse effects of the vaccine that are not currently known.”
Further, none of the vaccines have been subject to proper trials. Many of them skipped early-stage trials entirely, and the late-stage human trials have either not been peer-reviewed, have not released their data, will not finish until 2023 or were abandoned after “severe adverse effects”.
Vaccine manufacturers have been granted legal indemnity should they cause harm
The USA’s Public Readiness and Emergency Preparedness Act (PREP) grants immunity until at least 2024.
The EU’s product licensing law does the same, and there are reports of confidential liability clauses in the contracts the EU signed with vaccine manufacturers.
The UK went even further, granting permanent legal indemnity to the government, and any employees thereof, for any harm done when a patient is being treated for covid-19 or “suspected covid-19”.
Again, the leaked Albanian contract suggests that Pfizer, at least, made this indemnity a standard demand of supplying covid vaccines:
“Purchaser hereby agrees to indemnify, defend and hold harmless Pfizer from and against any and all suits, claims, actions, demands, losses, damages, liabilities, settlements, penalties, fines, costs and expenses.”
Covid “vaccines” carry a significant risk of adverse side effects
The experimental covid vaccines have potentially caused dozens of severe conditions in millions of people. These include myocarditis (especially in young boys), blood clots, allergic reactions, skin conditions, Bell’s Palsy, menstrual irregularities and more. [For a detailed breakdown of these conditions, read here]
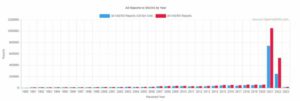
The US CDC’s Vaccine Adverse Event Reporting System (VAERS) has received twice as many reports since the covid vaccine rollout than all previous years combined.
Part VIII: Mortality Data
The survival rate of “covid” is over 99%
Government medical experts went out of their way to underline, from the beginning of the pandemic, that the vast majority of the population are not in any danger from covid.
A recent global review of covid data, published in October 2022 by Stanford epidemiologist John Ioannidis (et al) found a median fatality rate of just 0.07% in people younger than 70 years old.
Almost all antibody studies on the infection-fatality ratio (IFR) of covid have returned results between 0.04% and 0.5%. Meaning, assuming for a moment that “covid” ever existed as a discrete disease at all, its survival rate was at least 99.5%.
The vast majority of “covid deaths” have serious comorbidities
In March 2020, the Italian government published statistics showing 99.2% of their “covid deaths” had at least one serious comorbidity. These included cancer, heart disease, dementia, Alzheimer’s, kidney failure and diabetes (among others). Over 50% of them had three or more serious pre-existing conditions.
This pattern has held up in all other countries over the course of the “pandemic”. An October 2020 FOIA request to the UK’s ONS revealed less than 10% of the official “covid death” count at that time had covid as the sole cause of death.
In summary, the vast majority of “covid deaths” were very frail people.
This was interpreted by the press as old age or infirmity being “risk factors” for “covid”. However, it could be more accurately said that the number one risk factor for “dying of covid” was already dying of something else.
Average age of “covid death” is greater than the average life expectancy
The average age of a “covid death” in the UK is 82.5 years. In Italy, it’s 86. Germany, 83. Switzerland, 86. Canada, 86. The US, 78, Australia, 82. In almost all cases the median age of a “covid death” is higher than the national life expectancy.
Research from March 2021 found that, across the eight studied countries, more than 64% of all “covid deaths” occurred in people over the national life expectancy.
As such, for most of the world, the “pandemic” had little-to-no impact on life expectancy. Contrast this with the Spanish flu, which saw a 28% drop in life expectancy in the US in just over a year.
Covid mortality exactly mirrors the natural mortality curve
Statistical studies from the UK and India have shown that the curve for “covid death” follows the curve for expected mortality almost exactly:
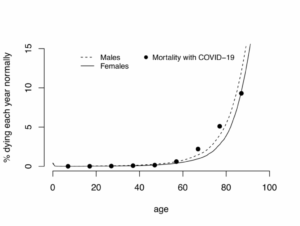
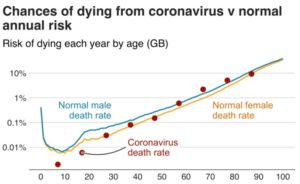
The risk of death “from covid” follows, almost exactly, your background risk of death in general.
The small increase for some of the older age groups can be accounted for by other factors.
There has been NO unusual excess mortality
The global death toll of “covid”, even with exaggerated statistics, was never high enough to justify the draconian responses we saw from most world governments.
In three years of “covid”, there have been roughly 6.8 million “covid deaths”, or 2.3 million per year. That’s 0.03% of the global population. For comparison’s sake, the Spanish Flu of 1918 killed 25-100 million people in two years, or between 0.7 and 2.8% of the global population per year.
The press has called 2020 the UK’s “deadliest year since world war two”, but this is misleading because it ignores the massive increase in the population since that time. A more reasonable statistical measure of mortality is Age-Standardised Mortality Rate (ASMR):
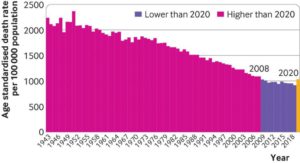
By this measure, 2020 isn’t even the worst year for mortality since 2000. In fact, since 1943 only 9 years have been better than 2020.
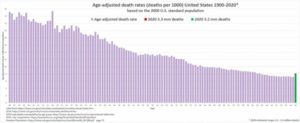
Similarly, in the US the ASMR for 2020 is only at 2004 levels:
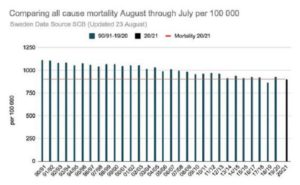
Sweden, which famously did not lockdown, saw their all-cause mortality hit levels previously seen in 2012:
The World Bank’s mortality dataset estimates that 2020 saw the crude global death rate increase from ~7.6 to 8, or a return to the level seen from 2006-2011.
From May of 2021, the World Health Organization began to discuss the “true cost of the pandemic”, promoting efforts to further inflate the pandemic’s death toll by attributing all excess deaths since 2020 to covid. However, since any increases in mortality could be attributable to non-covid causes that is either irrational or intentional deception.
Further, there is strong evidence any excess deaths had nothing to do with “covid”, since excess deaths have continued to increase even as Covid cases reportedly decline. As reported in the Spectator in November 2022: “Why are excess deaths higher now than during covid?”
It’s not just the UK either, as Toby Green and Thomas Fazi wrote for Unherd on January 30th: “Despite relatively low covid death rates, overall excess deaths in all age groups in Europe in 2022 were as high as in 2020 and higher than 2021 — even in the oldest cohorts. Beyond Europe, the situation is much the same.”
That excess deaths have continued to increase despite the “pandemic” allegedly slowing down is evidence that any excess mortality may never have been caused by “covid”, but was in fact due to other factors (e.g. the economic and social fallout of lockdown policies and potentially the distribution of untested and unnecessary “vaccines”).
Read the fourth part of the article
yogaesoteric
June 4, 2023