40 Facts You Need to Know: The Real Story of “Covid” (2)
Read the first part of the article
Part III: “Cases” and “Deaths”
Huge numbers of “Covid cases” are “asymptomatic”
Early in the “pandemic” it was reported that the majority of “covid cases” never exhibited any symptoms. In March 2020, studies done in Italy were suggesting 50-75% of positive covid tests had no symptoms. Another UK study from August 2020 found as much as 86% of “covid patients” experienced no viral symptoms at all.

A Chinese paper from March 2020 found over 80% of “asymptomatic cases” were actually false positive test results.
In short, the vast majority of “cases” during the first year of the “pandemic” were people who never got sick at all.
Following a WHO directive to re-test asymptomatic cases in January 2021 – just as the “vaccines” were first rolled out – the percentage of “asymptomatic cases” has been reportedly lower, approximately 40%.
“Covid case” numbers are inherently meaningless
From the onset of the “pandemic”, a “covid case” has been defined in terms guaranteed to artificially inflate statistics.
The World Health Organization’s definition of a confirmed case is anyone who gets a positive PCR result, regardless of symptoms or personal history. Further, it is known that many health agencies around the world – including the US CDC – include “probable cases” in their statistics.
The WHO defines a “probable case” as anyone who meets the “clinical criteria” (i.e. has flu-like symptoms) and has been in contact either a “confirmed case” OR another “probable case”:
“Probable Case: A patient who meets clinical criteria AND is a contact of a probable or confirmed case, or linked to a covid-19 cluster.”
As established above, PCR tests do not work and produce false positives. Lateral flow tests also produce false positives. It is known these tests may even give contradictory results for the same person at the same time. “Covid-19” also lacks a unique symptom profile, ruling out clinical diagnosis.
If you cannot reliably test for the disease in a lab, and cannot identify it via a unique symptom profile, and many “cases” are recognised as “asymptomatic”, then “covid19” becomes a label with no meaning.
Absent any kind of reliable diagnostic method, case statistics for any disease are inherently meaningless.
“Covid deaths” were created by statistical manipulation
Since “covid” case statistics are inflated it naturally follows that “covid” death statistics would be likewise unreliable. In fact it was noted from the very beginning of the “pandemic” that “covid death” counts were being artificially inflated.
According to the UK’s Health Standards Agency, the WHO defined a “covid death” in the following terms:
“A covid-19 death is defined for surveillance purposes as a death resulting from a clinically compatible illness in a probable or confirmed covid-19 case, unless there is a clear alternative cause of death that cannot be related to covid-19 disease (e.g. trauma).”
Throughout the “pandemic” many countries around the globe went even further and defined a “covid death” as a “death by any cause within 28/30/60 days of a positive test”.
Healthcare officials from Denmark, Italy, Germany, the UK, US, Northern Ireland and others have all admitted to this practice:
The US CDC even records “probable” covid deaths in their statistics.
Removing any distinction between dying of “covid”, and dying of something else after testing positive for covid will naturally lead to completely meaningless numbers of “covid deaths”.
British pathologist Dr. John Lee was warning of this “substantial over-estimate” as early as April 2020. Other mainstream sources have reported it, too.
Considering the huge percentage of “asymptomatic covid infections”, the well-known prevalence of serious comorbidities and the fact all “covid tests” are entirely unreliable, this renders the “covid” death numbers a completely meaningless statistic.
Part IV: Lockdowns
Lockdowns do not prevent the spread of disease
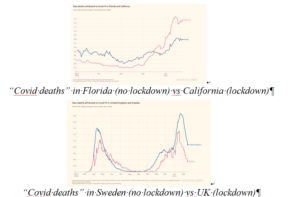
There is little to no evidence lockdowns have any impact on limiting “covid deaths”. If you compare regions that locked down to regions that did not, you can see no pattern at all.
A pre-print meta-analysis from Johns Hopkins University found lockdowns had almost no impact at all on “covid19” mortality, while another paper on the “Determinants of Covid-19 Fatalities” published in April of 2021 found “little evidence that lockdowns reduced fatalities”.
Lockdowns kill people
There is strong evidence that lockdowns – through social, economic and other public health damage – are deadlier than the alleged “virus”.
Dr. David Nabarro, World Health Organization special envoy for covid-19 described lockdowns as a “global catastrophe” in October 2020:
“We in the World Health Organization do not advocate lockdowns as the primary means of control of the virus, it seems we may have a doubling of world poverty by next year. We may well have at least a doubling of child malnutrition. This is a terrible, ghastly global catastrophe.”
A UN report from April 2020 warned of 100,000s of children being killed by the economic impact of lockdowns, while tens of millions more face possible poverty and famine.
Unemployment, poverty, suicide, alcoholism, drug use and other social/mental health crises are spiking all over the world. While missed and delayed surgeries and screenings have already seen increased mortality from heart disease, cancer and other conditions in many countries around the world.
A World Bank report from June 2021 estimated close to 100 million people had been plunged extreme poverty by so-called “anti-covid measures”.
As of January 2023, healthcare services the world over are still experiencing chaotic backlogs in treatment and diagnosis. The knock-on effects of lockdown will likely hurt public health for years.
The impact of lockdown could account for any observed increases in excess mortality.
Babies born during lockdown have lower IQs
A study done at Brown University found that children born after March 2020 had, on average, IQs 21 points lower than previous generations, concluding:
“Questions remain regarding the impact of the work-from-home, shelter-in-place, and other public health policies that have limited social interaction and typical childhood experiences on early child neurodevelopment.”
This mirrors reports in older children (aged 4-5) of stunted development of social skills and inability to read facial cues.
Hospitals were never unusually overburdened
The main argument used to defend lockdowns is that “flattening the curve” would prevent a rapid influx of cases and protect healthcare systems from collapse. But most healthcare systems were never close to collapse at all.
In March 2020 it was reported that hospitals in Spain and Italy were overflowing with patients, but this happens every flu season. In 2017 Spanish hospitals were at 200% capacity, and 2015 saw patients sleeping in corridors. A JAMA paper from March 2020 found that Italian hospitals “typically run at 85-90% capacity in the winter months”.
In the UK, the NHS is regularly stretched to breaking point over the winter.
As part of their covid policy, the NHS announced in spring of 2020 that they would be “re-organizing hospital capacity in new ways to treat covid and non-covid patients separately” and that “as a result hospitals will experience capacity pressures at lower overall occupancy rates than would previously have been the case.”
This means they removed thousands of beds.
Yes, during an alleged deadly pandemic, they actually reduced the maximum occupancy of hospitals.
Despite this, the NHS never felt pressure beyond your typical flu season, and at times actually had 4x more empty beds than normal.

In both the UK and US millions were spent on temporary emergency hospitals that were never used.
An article in Health Policy in November 2021 found that, in all of Western Europe, the “surge capacity” of ICU beds was exceeded for only one day – in Lombardy on April 3rd 2020.
There was a massive increase in the use of “unlawful” DNRs
Watchdogs and government agencies reported huge increases in the use of Do Not Resuscitate Orders (DNRs) in the years 2020-2021.
As early as March 2020, when the “pandemic” was still in its early stages, there were already papers appearing in mainstream journals predicting “unilateral” DNR usage, something which had “rarely had a role prior to covid”:
“Clinicians in some health care settings may unilaterally decide to write a DNR order. This latter approach is not uniformly accepted and, prior to covid-19, it rarely had a role. During this pandemic, however, in extreme situations such as a patient with severe underlying chronic illness and acute cardiopulmonary failure who is getting worse despite maximal therapy, there may be a role for a unilateral DNR to reduce the risk of medically futile CPR to patients, families, and health care workers.”
In the US, hospitals considered “universal DNRs” for any patient who tested positive for covid, and whistleblowing nurses have admitted the DNR system was abused in New York.
In the UK there was an “unprecedented” rise in “illegal” DNRs for disabled people, GP surgeries sent out letters to non-terminal patients recommending they sign DNR orders, whilst other doctors signed “blank et DNRs” for entire nursing homes.
A study done by Sheffield University found over one-third of all “suspected” covid patients had a DNR attached to their file within 24 hours of hospital admission.
A paper published in the journal Public Health Frontiers in May 2021, made the “ethical” case for “unilateral” use of DNRs in covid patients:
“Some countries were forced to adopt a unilateral DNR policy for certain patient groups. In the current difficult situation, difficult decisions are to be made. Societal rather than personal benefits might prevail.”
Blanket use of coerced or illegal DNR orders could account for any increases in mortality in 2020/21.
Part V: Ventilators
Ventilation is NOT a treatment for respiratory infections
Mechanical ventilation is not, and never has been, recommended treatment for respiratory infection of any kind. In the early days of the pandemic, many doctors came forward questioning the use of ventilators to treat “covid”.
Writing in The Spectator, Dr. Matt Strauss stated:
“Ventilators do not cure any disease. They can fill your lungs with air when you find yourself unable to do so yourself. They are associated with lung diseases in the public’s consciousness, but this is not in fact their most common or most appropriate application.”
German Pulmonologist Dr. Thomas Voshaar, chairman of the Association of Pneumatological Clinics said:
“When we read the first studies and reports from China and Italy, we immediately asked ourselves why intubation was so common there. This contradicted our clinical experience with viral pneumonia.”
Despite this, the WHO, CDC, ECDC and NHS all “recommended” covid patients be ventilated instead of using non-invasive methods.
This was not a medical policy designed to best treat the patients, but rather to reduce the hypothetical spread of covid by preventing patients from exhaling aerosol droplets, this was made clear in officially published guidelines.
Ventilators kill people
Putting someone on a ventilator who is suffering from influenza, pneumonia, chronic obstructive pulmonary disease, or any other condition which restricts breathing or affects the lungs, will not alleviate any of those symptoms. In fact, it will almost certainly make it worse, and will kill many of them.
Intubation tubes are a potential source of an infection known as “ventilator-associated pneumonia”, which studies show affects up to 28% of all people put on ventilators, and kills 20-55% of those infected.
Mechanical ventilation is also damaging to the physical structure of the lungs, resulting in “ventilator-induced lung injury”, which can dramatically impact quality of life, and even result in death.
Experts estimate 40-50% of ventilated patients die, regardless of their disease. Around the world, between 66 and 86% of all “covid patients” put on ventilators died.
According to an “undercover nurse”, ventilators were being used so improperly in New York, they were destroying patients’ lungs:
This policy was negligence at best and potentially deliberate murder at worst. This misuse of ventilators could account for any increase in mortality in 2020/21.
Read the third part of the article
yogaesoteric
June 1, 2023