The inanity of RNA vaccines for Covid-19 (II)
Read the first part of the article
To recap, we are experiencing a rather peculiar “pandemic” that exhibits:
– a case fatality ratio lower than the seasonal flu,
– kills less than the usual infectious diseases,
– didn’t trigger marked excess mortality and
– didn’t really lower life expectancy.

Existing treatment
Not only is covid-19 a benign disease, it can be cured by numerous treatments that are safe, effective and cheap: artemisia, high dose vitamin C, vitamin D, copper, zinc, doxycycline, fluvoxamine, bromhexine, colchicine, ivermectine, azythromycine and, of course, hydroxychloroquine. In addition, the combination of some of those drugs revealed beneficial synergies, in particular a cocktail of hydroxychloroquine + azythromycine + zinc. Notice also that the efficacy of the aforementioned drugs were published in peer-reviewed journals months ago.
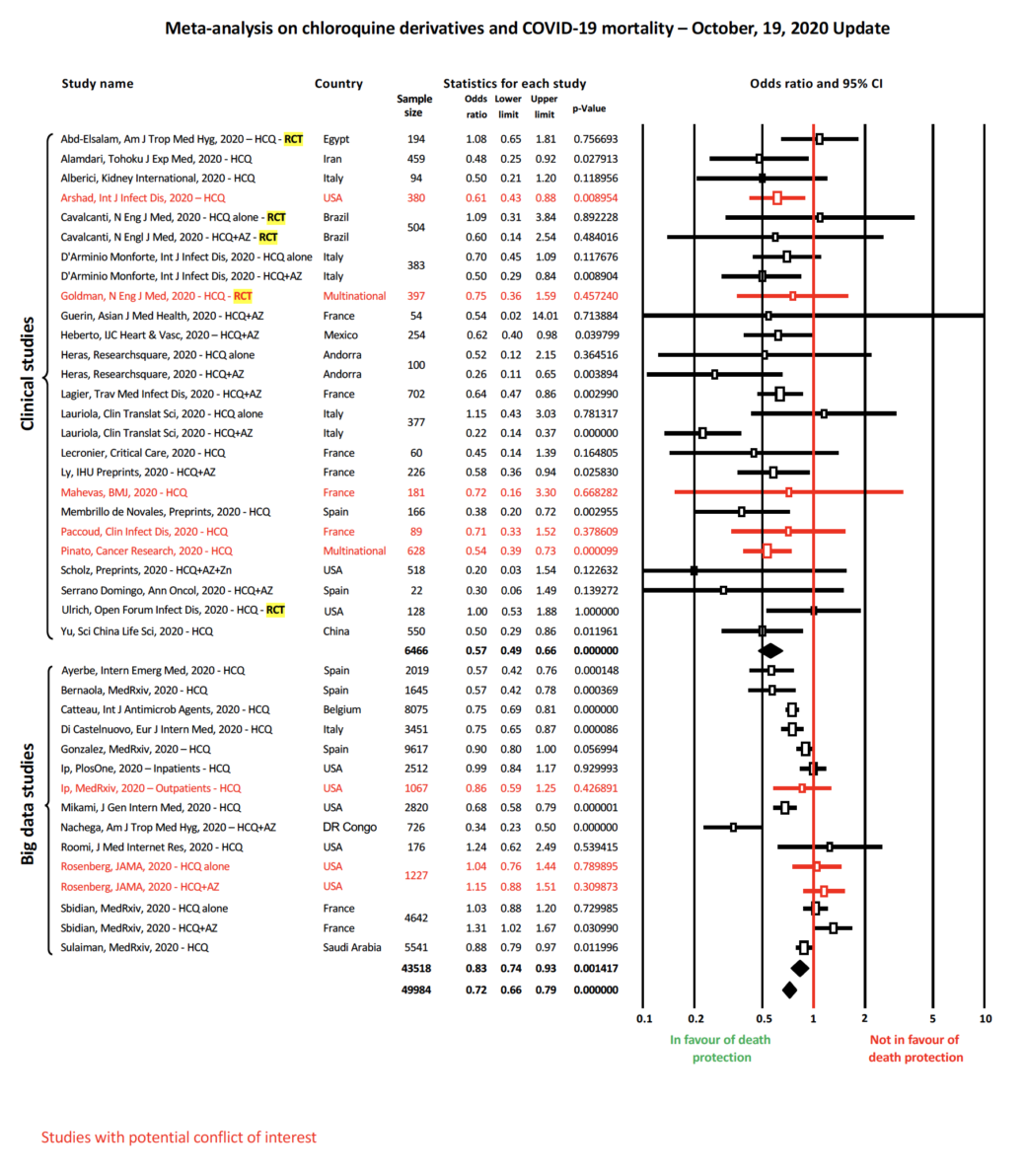
A case in point is hydroxychloroquine (HCQ) whose efficacy against covid-19 has been tested in no less than 195 published papers. The conclusion of the statistical meta analysis of those papers could not be clearer: “HCQ is effective for covid-19. The probability that an ineffective treatment generated results as positive as the 195 studies to date is estimated to be 1 in 1 quadrillion (p = 0.0000000000000009).” Another way to ascertain the efficacy of HCQ is simply to check if the research papers received funding from Gilead – the American-Israeli company, laden with conflicts of interests – that produces the now infamous Redemsivir. When there are conflicts of interest with Gilead, 73% of the papers claim that HCQ doesn’t work, if there is no conflict of interest, 83% of the papers conclude that HCQ works. It’s that simple.
Despite its repeatedly tested effectiveness, HCQ has been banned in a number of Western countries. In contrast, it took only one bogus paper, debunked soon after, for states to buy and administer billions of dollars worth of the toxic and ineffective Redemsivir.
The reason for the suppression of known treatments is at least two-fold:
– social: the denial of treatment to deliberately increase deaths and therefore fear in the population, leading to the reluctant acceptance of vaccines.
– legal: the accelerated FDA approval of a new drug is only possible when the targeted disease “has no cure”. The suppression of known cures enabled the Pfizer vaccine to go through an emergency FDA process which took only two months of limited testing and a meager trial report, while proper FDA approval requires about 12 years of extensive trials and a 100,000+ page new drug application.
To recap, covid-19 is a benign disease with numerous safe and effective treatments. In this context, the logical approach would be to increase the early clinical diagnosis and to spread and improve the existing therapeutic strategies.
That’s not what the elites decided, especially in the Western world. Instead they banned effective treatments and, among all kinds of dubious vaccines, enforced the worst one, the Pfizer RNA ‘vaccine’ on which the attention will be focused bellow.
Vaccine (mRNA vaccine) or gene therapy?
Despite its name, the Pfizer ‘vaccine’ is more akin to gene therapy, the definition of which is: “the utilization of the therapeutic delivery of nucleic acids into a patient’s cells”. The Pfizer ‘vaccine’ is exactly that, an artificial RNA sequence delivered via nano lipids into the patient’s cells, to hijack them and direct them to produce the spike protein found on SARS-CoV-2, or at least on one of its old variants. From there, the host should react to this protein by producing antibodies. Too many antibodies and an immune storm occurs, not enough antibodies and the triggered immunity is useless. Notice that gene therapy was never used on a large scale. It was only used in experimental phase 1 anti-tumoral protocols. The drugs were so toxic that phase 2 trials were never conducted. RNA “vaccines” against MERS and SARS followed the same path of failure. In 1999, geneticist Alain Fischer, conducted the first clinical trial with some rare positive results in the world of gene therapies. The same Alain Fischer was nominated as a vaccine expert by the French authorities. When asked about the Pfizer ‘vaccine’, Fischer answered cautiously, emphasizing that the effects of infectiousness and the duration of immunity were unknown, side effects were unavoidable and the fear of the vaccine was understandable. Obviously Fischer’s analysis didn’t fit the pro vaccine narrative, since then he no longer enjoys any media exposure.
Vaccine useless at best, detrimental at worst?
The history of vaccines is replete with major scandals. Here are a few examples:
1/ the Salk polio vaccine which caused the worst polio outbreak in history, infecting 200,000 people with live polio, of whom 70,000 became sick
2/ the current prevalence of poliomyelitis is caused by vaccines compared to naturally-occurring poliomyelitis
3/ the Dengue vaccine, triggering the production of antibodies that are not detrimental but beneficial to the Dengue virus, is leading to more severe forms of Dengue fever.
4/ and the recent case of Bergamo, Italy where the population experienced a high prevalence of severe forms of covid-19 among vaccinated people. There’s no mystery there, because for years, the flu vaccine has been known to favor and worsen coronavirus infections.
Likewise, vaccines against close relatives of SARS-COV-2 like SARS or MERS, that target the spike protein like the Pfizer ‘vaccine’, have also been tested but quickly canceled, one major adverse effect was the creation of antibodies that didn’t prevent but favored viral infections.
The vaccines against Dengue fever, influenza, SARS and MERS share the same fundamental flaw, which is well known by scientists as antibody-dependent enhancement, where the vaccine, instead of providing immunity, increase vulnerability and the severity of the disease it targets. In this context, it would not be surprising that the RNA vaccines trigger more severe forms of covid-19.
In addition, like most retroviruses, SARS-CoV-2 is very prone to mutations. The analysis of 10,000 of its genomes revealed a high number of genetic modifications: 2969 missense mutations, 1965 synonymous mutations, 484 mutations in the non-coding regions, 142 non-coding deletions, 100 in-frame deletions, 66 non-coding insertions, 36 stop-gained variants, 11 frameshift deletions and two in-frame insertions. This substantial number of genomic variation has led to the emergence of, at least 14 distinct variants, including the ‘English variant’ which displays 23 detectable mutations, 70% of them being located on its spike protein, which is the very target of the Pfizer ‘vaccine’.
Coincidentally, or not, the above mentioned Remdevisir has been tested on British patients in at least 15 different health centers and widely administered after its bogus approval. Redemsivir is now known to trigger mutations in SARS-COV-2, particularly in its spike protein. Given its mutagenic property and its use in the UK, the obvious question is “Did remdesivir play a role in the apparition of the English variant?”
In any case, just in Marseilles no less than 33 documented cases of patients fell sick twice, from the variant called Marseille 1, then from the variant Marseille 4. Worse than that, still in Marseilles, one patient got infected three times with SARS-CoV-2 variants in just nine months. Marseilles is no exception, in Manaus, Brazil the first epidemic of covid-19 conferred virtually no immunity against subsequent variants: between 44% and 66% of the population of Manaus was infected with SARS-CoV-2 by July […] Data show that >70% of the population had been infected in Manaus about 7 months after the virus first arrived in the city.
Reinfection with SARS-COV-2 is so widespread that scientists do not wonder any more if it happens, but how it happens: the possibility of reinfection with SARS-CoV-2 is not well understood. […] previous exposure to SARS-CoV-2 does not necessarily translate to guaranteed total immunity. The implications of reinfections could be relevant for vaccine development. […] Genomic analysis of SARS-CoV-2 showed genetically significant differences between each variant associated with each instance of infection.
Those reinfections suggest that natural immunity against COVID-19 could last just a few months, untill the person meets a different cov, one reason for this short immunity is the numerous mutations of SARS-CoV-2. But it is important to mention, as many scientists have already shown, that the natural immunity acquired against the viral strain which caused the disease you passed through, remains for life. The problem are the mutations that the virus encounts. If natural immunity doesn’t prevent a quick re-infection with another strain, the Pfizer ‘vaccine’, that, unlike natural immunity, only targets a small part of the virus – namely its spike protein, which has substantially changed (because of the mutations) since the design of the vaccine – should exhibit even poorer results. In conclusion, the Pfizer ‘vaccine’ is unlikely to confer lasting immunity, if any, especially against current and future variants.
The above is not just theory. For example in Israel no less than 12,400 residents have tested positive for SARS-COV-2 after receiving the Pfizer ‘vaccine’, among them 69 people who had already gotten the second dose.
Pfizer vaccine methodology
 1/ Irrelevant investigation objectives
1/ Irrelevant investigation objectives
A stunning bias in the Pfizer trial was its primary objective: evaluate the frequency of mild to severe forms of covid-19, 28 days after the first inoculation. Casualty rate, infectiousness, duration of immunity (if any), or even occurrence of mild to severe forms in the long term were not investigated. But the whole pandemic and vaccine hysteria were built on these very fears of death and contamination, we heard ad nauseam the media injunctions: “people are dying in droves”, “get vaccinated to avoid infecting others”, “get vaccinated to be immune to covid-19”, “get vaccinated to avoid dying of covid-19” etc.
2/ Tested group bias
Another striking bias is the trial selection, particularly the age combined with health status. It have been shown above that frail and elderly people are by far the most likely to suffer from covid-19. But only 2% of the Pfizer trial includes patients over 75 years old and with pre-existing medical conditions. In addition subjects of any age with comorbities are grossly under-represented. In total, only one out of five of the people appear to have an underlying condition, and for the various individual underlying conditions, the percentage of people suffering from them is often less than 1%.
Also the limited size of the vaccine group (about 20,000 participants) does not exhibit all the age/race/sex/disease/treatment/genetic profile combinations that the general population does. There is no safety data whatsoever about children, immune-compromised individuals or pregnant women because they were excluded from the trial.
Basically, Pfizer selected young and healthy subjects for testing a vaccine that is now administered as a priority to old and sick individuals. What is the point of studying healthy young individuals, who, vaccinated or not, are barely affected by covid-19 anyway? Does this bias minimize side effects and maintain the illusion of a safe ‘vaccine’?
3/ Placebo instead of known effective drugs
A new drug is tested against a placebo when the targeted disease has no known cure. In the case of covid-19, there are several known cures to which Pfizer should have compared its vaccine.
That was the design of the Discovery clinical trial that compared Remdesivir, HCQ and other drugs. When the preliminary results started to show that HCQ was the most effective, it was quickly removed from the trials. Pfizer didn’t make the same mistake of testing its new drug against an effective one. Instead, they tested their ‘vaccine’ against a placebo.
4/ Unilateral design and treatment of data
No third party was involved in the design of the trial, its monitoring, and the treatment of the results. The whole study was designed, conducted, analyzed, published and paid for by Pfizer itself. As Dutch neurologist Jan B. Hommel said: “The fact that an independent data and safety committee was able to see the data doesn’t change this, simply because they had no say in the design of the research, selection of the participants, the statistics used or the publication. … I don’t need to explain here how such a construction can lead to biased results of scientific research, because it has been extensively researched and published about over the past twenty years.”
Benefits
The main marketing argument for the Pfizer ‘vaccine’ is its alleged 95% efficacy. This figure is the sole claim of Pfizer and it should be taken with a grain of salt because of numerous factors:
1/ Pfizer precedent
First we have to understand the background of the company we are dealing with here. Pfizer is the world’s largest pharmaceutical company and it is also the company that has been hit with the second biggest criminal fine in US history for lying about one of their drugs and bribing doctors. This record fine is only one example.
Pfizer has been sentenced numerous times for covering up major side effects of Protonix, hiding the cancer-inducing properties of Prempro, lying about the suicidal behavior induced by Chantix, promoting Depo-Testosterone as effective and safe while it was ineffective and induces major side effects, and conducting illegal clinical trials for Trovan in Nigeria killing 11 children. The list of crimes committed by Pfizer goes on and on.
Let’s also keep in mind that Pfizer will cash in $14 billion a year, more than the GDP of Nicaragua, from the worldwide sale of its RNA ‘vaccine’.
2/ Relative efficacy VS absolute efficacy
During the Pfizer clinical trial 8 covid-19 cases were found in the vaccine group of 20,000 and 86 cases in the placebo group of 20,000. This means the attack rate for covid-19 is 0.0004 in the vaccine group and 0.0043 in the placebo group. Therefore, the absolute risk reduction for an individual is only about 0.4% (0.0043-0.0004X100).
The Number Needed To Vaccinate (NNTV) = 256 (1/0.0039), which means that to prevent just 1 Covid-19 case, 256 individuals must get the vaccine; the other 255 individuals derive no benefit, but are subject to the numerous adverse effects of the ‘vaccine’.
3/ Exclusion of suspicious cases
The claimed 95% (relative) efficacy was attained by excluding 3410 total cases of suspected, but unconfirmed covid-19 cases (probably due to false negatives). When those 3410 suspected cases are reintegrated the relative efficacy drops to 19% (which is well below the 50% effectiveness threshold set by regulators) and the absolute risk reduction drops to a ridiculous 0.08%.
4/ Non-replicated results
The cornerstone of any scientific work is its replicability. The results of the clinical trial were published in a journal at the end of 2020, but the clinical trials have not been replicated and they are unlikely to be replicated because no pharmaceutical company will conduct pricey clinical trials for a molecule patented by a competitor. So all we have is the word of Pfizer, who we also see is a repeat offender.
In summary, according to Pfizer, the benefit of its vaccine is a reduction of flu like symptoms in the young healthy population. They don’t know, or rather, they don’t want us to know, about what really matters: symptoms in the frail and elderly, mortality, infectiousness, or duration of immunity. We’re starting to get an idea.
The irony is that the ‘vaccine’ didn’t even reach its primary (and irrelevant) objective that was the reduction of the severe form of covid-19. In the editorial of the NEJM where the results of the Pfizer clinical trial were published, one can read: “The number of severe cases of covid-19 (one in the vaccine group and nine in the placebo group) is too small to draw any conclusions about whether the rare cases that occur in vaccinated persons are actually more severe.”
Read the third part of the article
yogaesoteric
July 10, 2021