What Moves Water Inside the Body? (2)
Untangling the Mysteries of Life, Aging and Spike Protein Injuries
Read the first part of the article
Mysteries of Microcirculation
A consistent pattern emerges when each circulatory pathway is looked at in the body. Tiny spaces with no extrinsic force driving their flow (or only a very small one) simultaneously require a regular movement occurring through them, and without that flow, life cannot function.
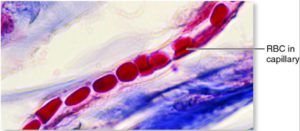
Note: in many cases, the blood vessels red blood cells travel through are smaller than the red blood cell, which requires the blood cell to deform to fit in the vessel—something which could not occur without some type of substancial force pushing the blood cell forward.
The immediate thought I had when I reviewed the anatomy of each was, “impairing physiologic zeta potential would be devastating here as any of the fluid in it would cease to flow it were to be clumped together.”
Note: one common way colloidal aggregations (from poor zeta potential) are dispersed is with mechanical force, as once they start flowing (due to a property known as thixotropy) they no longer clump together. Unfortunately, that means of dispersion is not available in tiny vessels which lack a circulatory pressure from a strong pump like the heart, and likewise explains why once the flow does stop it often cannot resume.
Many have also wondered what makes this microcirculation possible. Rudolph Steiner, for example, an Austrian mystic who made a variety of observations about the natural world that inspired generations to follow his work insisted that the heart was not a pump.
Because of this, countless doctors who follow his work have looked for evidence challenging the notion the heart is a hydraulic pump that moves the entire circulatory system. They, in turn, have identified a variety of observations that suggest pressure generated by the heart is not the driving force of circulation; instead, something independent of the heart’s pumping action causes blood to move throughout the body.
For example, spontaneous circulation can be observed in a developing embryo before the development of its heart, and the flow and pressures observed in the body are frequently inconsistent with the pressure the heart generates being the driving force behind blood circulation.
Note: many of these observations are detailed in this long-forgotten paper.
When I’ve thought this question over at length, it does not seem realistic that the heart could provide enough force to move the red blood cells through every capillary in the body. What then could be causing the fluids inside the body to move?
Proton Induced Motion
Pollack and his team made a chance discovery in their laboratory (discussed in great detail within this paper), which at last provided an answer to the mysteries of circulation.
“Fluid commonly flows in response to an external pressure gradient. However, when a tunnel-containing hydrogel [which contains liquid crystalline water] is immersed in water, spontaneous flow occurs through the tunnel without any pressure gradient. We confirmed this flow in a wide range of plant and animal-derived hydrogels. The flow appears to be driven by axial concentration gradients originating from surface activities of the tunnel wall. Those activities include (i) hydrogel-water interaction and (ii) material exchange across the tunnel boundary.”
As stated above, liquid crystalline water requires ambient infrared energy and a polar surface to form on. A curious phenomenon then occurs when that surface lines the inside of a tube (which, as far as I know, is the case for every fluid vessel in the body)—the liquid crystalline water lining the tube causes water to flow spontaneously through it.
“EZs [regions of liquid crystalline water] were studied previously by immersing sections of tubes made of a strongly hydrophilic material, Nafion, in aqueous microsphere suspensions. A microsphere-free EZ developed adjacent to the tube surface. In the central core of the tube, the movement of the microspheres demonstrated a flow, continuously sustaining itself at a velocity of ~10 μm/s in the axial direction [from the start to end of the tube]. Similarly, EZ and flow were also observed in tunnels lodged within various hydrogels. The gel materials included polyethylene glycol, poly(vinyl alcohol), and poly(acrylic acid). On the other hand, flow was not observed in tubes built of hydrophobic materials such as Teflon [and others], which do not generate EZs. The presence of EZ appeared to be a necessary condition.”
Since liquid crystalline water’s formation requires ambient radiant energy to form (e.g., the infrared energy present in light), its presence was found to influence the flow that was observed.
“We found that increased infrared energy substantially increased the flow velocity (Fig. 3B).
Since incident radiant energy (light) fuels EZ expansion, that energy may likewise fuel the self-driven flow. We confirmed that application of ultraviolet-containing white light could boost flow velocity by up to 500%. Thus, the self-driven flow mechanism can convert radiant energy into kinetic energy.”
Pollack theorized this flow was generated by the mutual repulsion created between the positively charged protons (hydrogen atoms) that are expelled as water (H2O) transitions to liquid crystalline (H3O2) water.
Note: that formation process is further explained here.
A few additional observations support this hypothesis. The first is that protons are continually added to the water that passes through:
“We found that the exiting water had a lower pH value than the entering water; the pH difference exceeded one unit and never diminished — even after 30 minutes of continuous flow. While we still couldn’t resolve the quantitative issue, we did establish that the passing water continued to receive protons from the annular EZ without diminution, even over extended periods of time.”
Note: In subsequent experimental designs, Pollack has demonstrated this flow can persist for hours to days.
The second was that flow was the greatest in narrow tubes:
“Another prediction of the proton-gradient hypothesis is that the flow should be faster in narrower tunnels. Assuming the proton-release rate per unit area of the annular EZ is spatially invariant, then, since reduced tunnel diameter means increased surface-to-volume ratio, a narrower tunnel should lead to a higher proton concentration in the core (see Fig. 3A). This results in a higher proton gradient (assuming the bath’s proton concentration remains unchanged), which, in turn, should lead to faster flow in the narrower tunnels.”
Note: narrow blood vessels are the most vulnerable to their blood flow being disrupted by an impaired zeta potential and hence where the initial subtle signs of illness often appear. It thus is remarkable the proton induced flow directly counteracts this vulnerability of the circulatory system.
The third was that the direction flow was always from the narrower end of a tube to the wider end:
“A common feature shared among the various flows was the direction—always toward the region with larger cross section or volume.
Thus, when a narrower tunnel lies in series with a wider tunnel, the proton gradient should point from the narrower to the wider section, as consistently observed.”
Likewise, in each case where it can be observed, each fluid conduit in the body is lined with a material recognized to create liquid crystalline water. For example, all blood vessels, including the smallest capillaries, are lined with a protective glycocalyx, and the glycocalyx is remarkably well suited for creating liquid crystalline water on its surface (which Pollack and others have verified is indeed there).

The biological flow of fluids that is independent of a central pump has also been explored in animals:
“On the other hand, blood can apparently flow without a beating heart. After the heart had been arrested, postmortem blood flow was confirmed in mice, rats, dogs, and chick 30 embryos (4-7). The flow persisted from 15 minutes to several hours. Furthermore, some 31 amphibian larvae could live up to 15 days, and even differentiate following surgical 32 removal of the heart (8-10), implying an alternative means for propelling blood.
Here, in an avian circulatory model, we confirm several predictions arising from this flow mechanism. First, flow continues after cardiac ejection has been stopped; this implies some driving mechanism beyond ventricular ejection.
Second, IR energy fuels this flow, both in the post-mortem situation and also in the normal physiological state. All of this demonstrates the existence of a second driver of blood flow, beyond the heart: the vessels, themselves.”
Other organisms also utilize this mechanism. Plants require significant internal transportation of water (e.g., consider how high trees must pull water from deep underground to sustain themselves) but do not have any pumping organ which could facilitate this activity.
“To explore the generality of the self-driven flow, we tested diverse hydrogels. They comprised plant-derived hydrogels including agarose, agar, and starch, as well as animal-derived hydrogels including collagen and gelatin. These hydrogels, ranging from polysaccharides to proteins, were chosen on the basis of their broad appearance in nature and wide application in science and technology.”
In the lab, Pollack demonstrated that the xylem (the vessel plants use to transport water) creates liquid crystalline water. Pollack has also shown that the flow created by liquid crystalline water allows it to overcome the resistance of gravity and climb up tubes (a commonly observed phenomenon known as capillary action).
Additionally, Pollack has also demonstrated that the random spontaneous particle movement observed in water (known as Brownian motion) is influenced by light. This suggests it is likely due to the motion created by liquid crystalline water (which light drives the formation of). Unlike the tube examples discussed in this section, where something exists to direct the flow created by the charge repulsion between hydrogen atoms, in most cases, that structure is not present, and random motion instead occurs.
Direction of Circulatory Flow
Pollack’s model shows that the liquid crystalline water goes from the area of highest to lowest proton gradients, which, in most cases, means going from a narrower to a wider conduit. This is important for another reason—it mirrors the direction of fluid flow in the body in areas with minimal to non-existent pumping mechanisms. This again suggests the utilization of liquid crystalline water is fundamental to the body’s design.
For example, when blood exits the smallest blood arteries and enters the capillaries (where much of it leaves the circulation to nourish the tissues), it needs to then flow into the smallest veins, which merge into a much larger and more powerful flow as the veins join together into larger and larger veins. At the capillaries, no pressure exists to serve as a pump, yet the power behind the circulation never stops, so something else needs to be at work.
Since the smallest veins are three times the size of the smallest arteries (and continue expanding), a natural direction of flow from the smallest arteries to veins is created. Similarly, the lymphatic system (which has a variety of weaker pumps recognized to fail in various complex illnesses) also starts off as tiny lymphatic vessels that eventually collect in much larger lymphatic vessels.
At the same time, however, since most of the arterial flow goes from larger to smaller vessels, the picture is a bit more complex and required Pollack to test it directly.
“As the model predicted, the flow in the large, near-heart arteries was indeed opposite to the natural direction just after the heart stopped beating. Hence, model predictions appear to match experimental observations for all vessel beds [this implies the hearts contractions does plays a key role in the direction of arterial blood flow].
If the flow in arteries is against the flow in the capillaries and the veins, a natural question is: who plays the dominating role? The answer should be the capillaries and the veins: compared to the arterioles, the venules [smallest veins] are higher in number; thus, more venules can generate flow. This conclusion is verified by the dynamics of the postmortem arterial blood flow. Postmortem flow in larger arteries was originally in the reversed direction, not the natural direction. Yet, the flow gradually resumed its natural direction from the peripheral region of the arterial network, indicating that the blood flowed into the capillaries and the veins. As the non-beating heart stopped replenishing blood to the arteries, ultimately, the arteries emptied. The emptied arteries indicate that the flow driving capacity of capillaries and veins exceeds that of the arteries. Thus, all blood vessels drive the blood towards the natural direction.”
Liquid Crystalline Water and Zeta Potential
Many of the factors which influence the formation of liquid crystalline water also influence the physiologic zeta potential. After looking at each factor for an extensive period of time, I concluded:
- Colloidal systems can either depend upon a mutual negative or mutual positive charge to maintain the repulsion necessary to ensure colloidal stability. In nature, in almost all cases, this is done with negative rather than positive charges. I believe this is due to the negative charge liquid crystalline water inherently creates around polar surfaces in water (which hence necessitates everything else also being negatively changed so that they repel from each other).
- In most cases, the same factors which promote the formation of liquid crystalline water also promote a more negatively charged physiologic zeta potential and the stabilization of proteins in solution (rather than them being “salted out”).
- In many cases, it’s likely the mechanisms are being mixed up, and the change an agent is observed to cause in one parameter is actually due to it changing a different linked parameter (e.g., some of the agents which “restore the physiologic zeta potential“ are actually enlarging the liquid crystalline layer around colloidal particles in the solution and hence creating the appearance of altering the physiologic zeta potential because particle dispersion increased).
The Spike Protein and Zeta Potential
In late 2019, I realized covid would turn into a huge problem. Because of this, I contacted my colleagues who, unlike me, were practicing in areas I expected to be hard hit by it (e.g., New York City) and once covid started within the United States, they were willing to share their clinical observations. One of the aspects I heard repeatedly was reports suggesting abnormal stagnation was occurring in the fluids of their patients.
For context, we hold the beliefs that one of the most common aspects that is observed in hospitalized patients is an impaired physiologic zeta potential. Furthermore, long ago, it was demonstrated that people who had pre-existing impairment of their zeta potential were far more likely to have heart attacks or be hospitalized, and that the small decrease in zeta potential infections like the flu could create, while inconvenient for most, could be devastating for those with an already impaired zeta potential (as it dropped them below a critical threshold). Likewise, we also believe that the routine treatment reflexively given to most hospitalized patients, intravenous fluids actually “works” because it partially restores the physiologic zeta potential.
Note: One of the best recent pieces of evidence I heard for this theory was Pierre Kory’s observation that occasionally, bedside ultrasound in the critical care unit would show the blood in the largest veins of the body will is clumping together and that this sign typically immediately precedes death. This observation mirrors what investigators over 50 years ago found in monkeys infected with malaria—that as the infection progressed, blood clumping would occur in larger and larger blood vessels. Once it occurred in the largest vessels, death would immediately follow (unless something was provided to prevent the clumping). This progression of blood clumping together first in the smallest and then eventually the largest vessels as disease severity increases also mirrors some of the classic diagnostic models within Chinese Medicine.
Many of the observations my colleagues on the early front lines of covid shared with me mirrored what I had previously associated with extreme disruptions of zeta potential, something which had not been observed with the original SARS virus (SARS-CoV-1). This then raised the question, why does SARS-CoV-2 cause that?
After looking at it for a while, I concluded it had to be the high positive charge density unique to the SARS-CoV-2 spike protein. This became the original reason for my concern with the vaccine. Since then, many signs have emerged that the spike protein directly affects zeta potential. These include:
- Modeling showing the SARS-CoV-2 spike protein adversely affects physiologic zeta potential.
- Some of the unusual characteristics of covid (e.g., the low blood oxygenation arising in the peripheral but not central vessels) being due to its zeta potential induced microclotting. One study supporting this link showed athletes who received the vaccine experienced a decline in their oxygen uptake.
- Some of the therapeutic benefits (e.g., from ivermectin or ozone) seen in hospitalized patients, such as improved oxygen uptake occurring immediately following treatment, something that likely can only be attributed to a rapid dispersion of blood clotting.
- Ivermectin being directly demonstrated to disperse spike protein-induced blood clumping (microclotting).
- Vaccine injured patients and “normal” vaccinated patients developing subtle cranial nerve palsy’s indicative of microstrokes having occurred. Many of the other symptoms commonly associated with covid vaccine injuries are also aspects I had previously learned to associate with poor zeta potential.
- People performing live blood cell analysis observing blood clumping occurring in vaccinated blood (e.g., see this study).

- Vaccine-injured patients improving from a variety of treatments directed at restoring physiologic zeta potential.
Conclusion
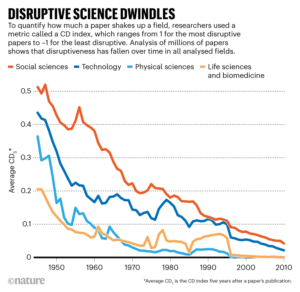
As the years have gone by, our system of science has become more and more influenced by commercial and political pressures, resulting in research more and more focusing on what can make money and protect existing interests rather than on what advances humanity.
In the case of medicine, this has resulted in research that incriminates business interests (e.g., by showing a pharmaceutical is toxic) being blocked. Likewise, research that provides economic means of treating illness and hence competes with the medical industry inevitably is blocked.
This obstruction has held particularly true for investigating the root causes of illnesses as if you have a simply scientific process that can account for many different diseases (e.g., colloidal agglomeration), it invalidates large swathes of disease markets. As such, most of our medical research focuses on the biochemical model of illness, a framework where each illness is viewed as the result of an issue with a specific protein that requires a unique (patentable) compound or antibody to interact with it, making it possible to create an almost limitless number of profitable pharmaceutical products.
Unfortunately, in many cases, this approach (beyond being extremely expensive) cannot provide the results or health people are looking for if the illness results from something else (e.g., an impaired physiologic zeta potential). Because of this, I believe that advancing medicine (and making it affordable again) will require us to re-examine many of our foundational conceptions of the body and asking if there is something else we are missing (or have forgotten) such as how water is moving in the first place. Fortunately, we at last appear to be entering an era where embracing these new paradigms may indeed be possible!
Author’s Note: there are three companion articles to this piece. The first, which describes the science of zeta potential and how it underlies many vaccine injuries can be read here. The second which discusses the methods that can be used to increase liquid crystalline water and improve the physiologic zeta potential can be read here. The third which describes what types of water we drink (as we’ve found appropriately purified waters that restore the physiologic zeta potential are often a very economical way to improve health) can be read here.
Author: A Midwestern Doctor
yogaesoteric
December 18, 2024