The inanity of RNA vaccines for Covid-19 (I)
Peculiar “pandemic”
The present article, using objective data, expose the characteristics of Covid-19 “pandemic”, the supressing of Covid-19 efficient therapy and many aspects of Pfizer vaccine.
In Compelling Evidence That SARS-CoV-2 Was Man-Made, published in June 2020, it is concluded: “It’s probable that by the end of 2020, like every year, a flu epidemic will emerge. This virus will, conveniently, be deemed a close relative to SARS-CoV-2, maybe with ‘extra terrifying features’.
But there will be no need to despair because, by this time, the authorities will have prepared a vaccine. That’s one of the reasons why hydroxycholoroquine was lambasted and banned. If a safe and effective treatment already exists, who is going to accept a rushed and unknown vaccine? A vaccine that will allegedly protect people against COVID-20, but will in reality be designed to ‘cancel’ the beneficial changes induced by the mutated strain of SARS-CoV-2. […]
It’s probable that the vaccination won’t be mandatory. Remember that the authorities are now “kinder and gentler”. Instead of brute force, the authorities are more likely to use moral blackmail – “Get vaccinated to protect others!” – combined with social blackmail – “No vaccine = no job, no shopping, no travel, no socializing!” Basically, you’re free to choose between the vaccine passport or a life sentence in an isolated cell.”
At present, as suspected, new cov variants have appeared, manufactured COVID-19 deaths are ‘piling up‘, the vaccine passport has already been adopted by several countries and vaccination campaigns have been launched around the world.
In theory, medicines, vaccines included, are approved and used because their benefits far exceed their risks. In this sense, the ideal medicine would display zero risks and total effectiveness against an uncured and deadly disease.
We’ll see in the present article that the COVID-19 vaccines, particularly the Pfizer vaccine, is pretty much the opposite of the ideal drug. It is dangerous, ineffective and targets a benign disease that already has known effective and safe treatments.
Where’s the pandemic?
Case Fatality Rate
According to the WHO (World Health Organisation), in October 2020 an estimated 750 million people – about 10% of the world’s population – had been infected by SARS-CoV-2, and one million people had died of COVID-19. Those figures lead to a case fatality rate (CFR) of 0.13%, which is the typical CFR exhibited by the seasonal flu. When treated properly, like in Marseilles – where a hydroxychloroquine-based protocol and early clinical diagnosis was used – the CFR drops as low as 0.05%. In Singapore, where the use of hydroxychloroquine is widespread and no national lockdown was ever imposed, the CFR of COVID-19 is the same as Marseilles, a mere 0.05% (29 deaths out of 59,000 cases).
What kind of pandemic exhibits a case fatality rate equal to, or lower than, seasonal flu?
Real COVID deaths
The numbers above are based on the official data published by the WHO. Those numbers, particularly the total COVID deaths, are grossly inflated due to various deceptions:
1/ Comorbidity:
94% of the people who died of COVID-19 had comorbidity (chronic disease/diseases at the time of cov infection) factors. A majority of them had not one but several comorbidity factors – in particular hypertension, obesity, chronic lung disease, diabetes and cardiovascular disease. For example a UK patient who had advanced cancer, kidney failure and diabetes, and had tested positive within 60 days prior to his death, will have his demise automatically attributed to COVID-19. In the UK, at the very least 30% of deaths attributed to COVID-19 are actually due to a comorbidity.
2/ False positives:
A lot of deaths were attributed to COVID-19 solely on the basis of a positive PCR test. In the words of its inventor Kary Mullis, chemistry Nobel Prize winner in 1993: “…[PCR tests] cannot detect free infectious viruses at all […] The tests can detect genetic sequences of viruses, but not viruses themselves.”
The obvious question, therefore, is: how many other entities display genetic sequences similar to SARS-CoV-2. PCR tests for SARS-COV-2 are based on 4 genes: RNA-polymerase (Rd-Rp), S gene (Orf2), E gene (Orf1ab) and N gene (Orf9a). The two first genes are found in dozens of human chromosomes and the two last ones are found in almost 100 different microbes. When these microbes and chromosomes sequences are detected, they are wrongly attributed to SARS-CoV-2.

The above is one reason for false positive test results, the other one relates to the number of PCR amplification cycles. According to the US CDC, it is virtually impossible to detect any live virus above a threshold of 33 cycles. However, many governments conduct 40, 45 even 50 amplification cycles. For illustration, a positive test at 40 cycles has about a 43% chance of no longer being positive, with a cutoff of 35, and 85% chance with a cutoff of 30. The antigen test is even worse than the PCR test, leading to 63% more false positives! These tests are so unreliable that even the WHO discourages their use.
3/ Ban of effective treatments:
In Marseilles, France, where early diagnosis and proper treatment – including hydroxychloroquine combined with azythromycin – are administered, the crude mortality rate is 0.01%. 400 miles from there, in Paris, where there’s late diagnosis and the ban on those two drugs is enforced, the overall mortality rate jumps up to 0.075%. That’s a 7.5 fold increase.
Similar to Marseilles, Belarus and Iceland administered proper care and/or conducted early diagnosis, and they are among the countries with the lowest number of COVID-19 deaths, with, respectively, 1,560 (0.016% crude mortality rate) and 29 (0.008% crude mortality rate) as of mid-January 2021. In the same vein, in Vietnam, which uses hydroxychloroquine, early diagnosis and implemented no national lockdown, crude mortality due to COVID-19 is 0.000036% (35 deaths among 96 million inhabitants).
4/ Transfer of flu casualties:
The southern hemisphere appears to have simply skipped the winter 2020 flu season, where flu deaths showed a 90% drop compared to previous years. According to mainstream media, this drop in flu deaths is due to the lockdown. If this is the case, however, how do we explain that France recorded a surprisingly low number of flu deaths during the flu season 2019-2020 that ended before the lockdown was imposed on March 17th. Indeed, only 3,680 flu deaths were recorded during the winter of 2019-2020. That’s a 70% drop in flu deaths compared to the last 10-year average mortality.
Another narrative explaining this sharp and unexpected drop in flu casualties is that the coronavirus prevented the activity of other viruses. But viruses have no difficulties in cohabiting. For example, in Europe alone during the 2019-2020 flu season, there were at least six active flu strains: type A/H1N1/pdm09, A/H3N2, A/Unknown, B/Victoria, B/Yamagata and B/Unknown – and we know that SARS-CoV-2 was on the continent since at least December 2nd 2019.
In the northern hemisphere, France was not the only country to experience the disappearance of its annual seasonal flu. The USA and the UK respectively reported a staggering 98% and 90% decrease in deaths attributed to the seasonal flu.
Starting with the hyper-inflated WHO number of COVID deaths, which is 1.7 million as of January 2021, we can deduce the following numbers:
– False positive deaths, patients who didn’t even have COVID, represent – at the very least – 33% of the total number of deaths attributed to COVID-19. That’s 700,000 out of 1.7 million.
– Deaths due to comorbidities represent 30% of the total number of deaths attributed to COVID. That’s 500,000 out of 1.7 million.
– About 90% of the typical flu death toll was transferred to the COVID tally. That’s 300,000 deaths out of 1.7 million.
Depending on the overlaps between those three kinds of non-COVID deaths, the real number of COVID-19 deaths can be estimated at between 300,000 and 1.1 million.
That range doesn’t even take into account the 7-fold reduction in mortality related to proper early diagnosis and adequate treatment.
Factoring this parameter in, the total mortality due to COVID-19 with early diagnosis and proper care would drop to somewhere between 40,000 and 140,000 casualties worldwide.
Notice that the estimates above are very conservative. We are therefore left to wonder whether SARS-CoV-2 actually directly caused a significant number of deaths at all.
What kind of pandemic induces much less total deaths than the seasonal flu?
Excess mortality
The excess mortality includes deaths attributed to COVID-19 along with the numerous deaths due to the lockdowns. As we will see, it is likely that lockdowns induced many more deaths than COVID-19.
1/ Delayed treatments and diagnosis
Only a third of the excess deaths seen in the care homes and private residences in England and Wales can be explained by covid-19, the remaining two thirds are due to elderly citizens who were denied primary care and “who may well have lived longer if they had managed to get to hospital“. This problem is particularly true for cancer patients. In the UK, the denial of cancer diagnosis and medical treatment may lead to 18,000 more cancer patient deaths.

2/ Psychiatric conditions
A meta analysis of the mental health of the general population was published in December 2020. As expected, the “pandemic” significantly exacerbated this situation: Relatively high rates of symptoms of anxiety (6.33% to 50.9%), depression (14.6% to 48.3%), post-traumatic stress disorder (7% to 53.8%), psychological distress (34.43% to 38%), and stress (8.1% to 81.9%) are reported in the general population during the COVID-19 pandemic in China, Spain, Italy, Iran, the US, Turkey, Nepal, and Denmark […] The COVID-19 pandemic was associated with “highly significant levels of psychological distress that, in many cases, would meet the threshold for clinical relevance.” It should be noted that the life expectancy of individuals suffering from mental illness is about 8 years shorter than the general population.
3/ Suicide
The definitive numbers about deaths in 2020 have not been compiled yet. However, the trend is already clear. According to some studies, suicide increased by 145%. Logically, suicidal tendencies surged alongside actual suicides with, for example, India experiencing a 67.7% increase in reports of suicidal behavior during lockdown. Similarly, in China, the appearance of very frequent suicidal thoughts has been noted, while in Canada a 500% increase in suicide is projected.
4/ Alcoholism and drug addictions
Alcohol abuse sharply increased during the “pandemic”. In the UK, there was a 500% rise in calls to the British Liver Trust helpline since lockdown began in March 2020. Similarly, Alcohol Change recorded a 242% rise in visits to their advice and support pages on their website during lockdown. Surveys on alcohol consumption tell a similar tale, with 21% of individuals stating they were drinking more often during lockdown. The heavy drinkers were the most affected, 38% of those who typically drank heavily during pre-lockdown said they drank even more during lockdown. In the US, a 54% increase in national sales of alcohol was recorded for the week ending March 21, 2020, compared with the previous year.
Similarly, drug overdoses rose strongly in 2020. For example, in the US, overdoses killed a staggering 81,000 people, a 38% increase in fatal overdoses compared to 2019.
5/ Poverty
According to the Worldbank, the “pandemic” could throw about 100 million additional people into extreme poverty. The difference in life expectancy between an individual in extreme poverty and a wealthy individual is at least 20 years. Notice that most of the deaths induced by the surge in extreme poverty will not happen immediately but in the years, if not decades, following this manufactured global economic crisis.
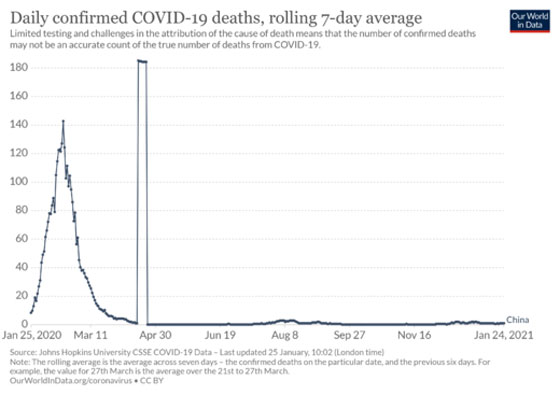
Despite the number of deaths due to lockdowns and their consequences rather than COVID-19, many countries didn’t even see a rise in excess mortality during the so-called pandemic. That is the case in Germany where hydroxychloroquine was used and a lot of early diagnosis was done. Better than that, Iceland – which implemented one of the most effective early diagnosis approaches in the world – shows a mortality rate in 2020 that is lower than its average yearly mortality. But the cherry on the cake is China, where about 55 tons of hydroxychloroquine were consumed in 2020 and where no national lockdown was implemented: as a result, China experienced virtually zero COVID deaths since April 2020.
Even France, which banned hydroxychloroquine and azythromycin and implemented extended lockdowns and curfews, experienced a mortality rate during Spring 2020 that was lower than during the 2017 flu season and since May 1st, 2020, no increase in mortality has been noticed.
What kind of pandemic doesn’t cause a marked excess in mortality?
Life expectancy
In France, even before they tested positive for the virus, 80% of alleged COVID-19 victims had a life expectancy lower than one year due to comorbidities and advanced age. Overall, COVID-19 victims had a life expectancy of a mere 3 years and 82% of the victims were more than 70 years old. The average age for a COVID-19 death is 82, that is a few months shorter than the overall life expectancy. In several countries, the average age of deaths attributed to COVID-19 is even higher than life expectancy. For example, in the UK, the average age for COVID-19 death is 82,6 years old while the average life expectancy is 81.2 years. In Sweden, the average age of those who have allegedly died of COVID-19 is 84 years old, two years more than the average age of death which is 82.
As a result of the very advanced age of the people who allegedly died of COVID-19, many countries didn’t experience any drop in life expectancy. This is the case in China that recorded 4,600 deaths attributed to COVID-19 out of a population of 1.4 billion, or Iceland and its 19 COVID victims out of 400,000 Icelandic citizens.
Even in France, where a lot of elderly citizens were left to die in nursing homes, where drastic lockdowns were implemented, where diagnosis and care was delayed for serious conditions and effective medicines against COVID-19 were banned and toxic drugs like Rivotril or Remdesivir were administered instead, life expectancy only decreased by 5 months.
What kind of pandemic doesn’t notably decrease life expectancy?
In summary, the typical victim of COVID-19 is an individual in his 80’s who lives in a nursing home and has several comorbidities. Typically, such a person died because of the despair of social isolation and the delayed diagnosis and treatment of his serious comorbidities. In many cases, the patient didn’t even have COVID-19. However COVID-19 killed him, not directly, but through the isolation and denial of care induced by the well-orchestrated pandemic hysteria.
To recap, we are experiencing a rather peculiar “pandemic” that exhibits:
– a case fatality ratio lower than the seasonal flu,
– kills less than the usual infectious diseases,
– didn’t trigger marked excess mortality and
– didn’t really lower life expectancy.
Read the second part of the article
yogaesoteric
June 30, 2021