NHS Dr reveals Staff were ordered to “Euthanise” Patients to fraudulently increase Covid Death Count because Hospitals were Empty & Nurses were having TikTok Dance-Offs
An NHS whistleblower, who wishes to remain anonymous, has come forward with allegations that the NHS hospitals were not overwhelmed during the covid-19 pandemic, as was reported by authorities and the mainstream media.
The whistleblower also confirmed that the little care given throughout the pandemic amounted to negligence, and that the government and NHS bosses essentially instructed staff to let people die, or in some cases kill them through the ‘End of Life Care’ programme and falsely label the deaths as being due to covid-19.

This person referred to as Dr. John has worked in minor injuries and illness centres as well as in a primary care role throughout the pandemic.
Dr. John claims that he has “seen this mess evolve from the very beginning of the pandemic” and that hospitals were actually extremely quiet and almost empty during the first lockdown.
“I used to see an average of 20 patients per day, that dropped to 1 – 2 patients during the first lockdown. I have even witnessed an elderly lady with horrific broken bones come into the hospital three weeks after her accident as she was too scared of catching coronavirus to visit the hospital sooner. In the end, the pain overcame the fear.
I have also assessed people with chest pains in their homes who would not go for further assessment as they were so scared of ‘the virus’ they would rather chance a heart attack than the infection or the loneliness of going to the hospital alone.”
NHS statistics certainly back up Dr John’s claims.
Alternative media examined the data for A&E attendance in the months of April (lockdown 1) and November (lockdown 2) for 2020 and compared this with April and November in 2018 and 2019 which showed A&E attendance during the first lockdown was 57% down on the previous year, and A&E attendance during lockdown 2 was 31% down on the previous year.
- 2018 – April – 1,984,369 attended A&E / November – 2,036,847 attended A&E
- 2019 – April – 2,112,165 attended A&E / November – 2,143,505 attended A&E
- 2020 – April – 916,581 attended A&E / November – 1,485,132 attended A&E
This significant drop in attendance suggests that people were too scared to visit the hospital due to the fear propaganda perpetuated in the mainstream media.
Furthermore, Dr. John also describes how changes in care policies have led to patients not receiving proper follow-up care, resulting in negative outcomes for patients and their families.
He states that usual follow-up visits were not done and parents were removing casts from their children’s broken limbs, “I dread to think the state of some of their limbs”.
He also mentioned that a change in care policies led to one 80+–year-old woman being permanently disabled.
He describes visiting an elderly patient who had only had a single face-to-face physio follow-up and a single phone follow-up after a hip operation. He found her in a bedridden state, unable to transfer to a commode, her dignity taken away.
The demise of the NHS didn’t just affect Dr. John’s patients though, it also affected him personally as he lost a family member to cancer during the alleged pandemic due to not being given the required care.
“He was given 7 years to live with his illness, he lasted just 1 year in the new NHS system.
I’ve also witnessed the desperation of families witnessing their own relatives dying sooner than they should have due to the lack of professional care that should have been provided. It has been a very sad year in which I have witnessed the demise of the health service.
I have also seen stroke patients sent home without being given any follow-up care. I also know of a triage policy in which staff were forced to send potentially seriously ill people home on the premise of giving them a call if their condition worsened”.
Dr. John’s claims are supported by a Care Quality Commission report that found 34% of NHS staff were pressured into placing “Do Not Resuscitate” orders on Covid patients with disabilities and learning difficulties. The policy led to people with disabilities and learning difficulties accounting for 3 in every 5 covid deaths according to official ONS figures.
This testimony from an NHS staff member suggests that the public was being lied to regarding the official narrative of the NHS being overwhelmed during the pandemic.
It highlights the terrible impact of misinformation and fear propaganda on the public’s perception of the situation, leading to people avoiding seeking medical treatment for fear of contracting the virus.
Additionally, it also highlights the horrific impact of changes in care policies, leading to patients not receiving proper follow-up care and terrible outcomes for patients and their families.
This fact is also backed up by a document nicknamed ‘The Death Document’ that was published by NICE, an executive non-departmental public body, sponsored by the Department of Health and Social Care.
There is also a mountain of evidence that the UK Government authorised the essential “mass murder” of the elderly and vulnerable by Midazolam injection and then told the public covid-19 was to blame.
Between 2 March and 12 June 2020, 18,562 residents of care homes in England died with covid-19, including 18,168 people aged 65 and over, representing almost 40% of all deaths involving covid-19 in England during this period.
This is a significant number considering that during the same period, 28,186 “excess deaths” were recorded in care homes in England, representing a 46% increase compared with the same period in previous years.
A number of decisions and policies adopted by authorities at the national and local level in the UK violated care home residents’ rights to life, to health, and to non-discrimination.
These include:
- Mass discharges from hospital into care homes.
- Imposition of blanket Do Not Attempt Resuscitation (DNAR) orders on residents of many care homes around the country and restrictions on residents’ access to hospital.
- Suspension of regular oversight procedures for care homes by the statutory regulating body, the Care Quality Commission (CQC), and the Local Government and Social Care Ombudsman.
These actions by authorities contributed to the high number of deaths among care home residents during the pandemic.
It is also stated that serious illness in covid-19 presents pneumonia and accompanying respiratory insufficiency.
Therefore, typical symptoms include breathlessness, cough, weakness and fever. It is also noted that people who suffer deteriorating respiratory failure and who do not receive intensive care, develop acute respiratory distress syndrome with severe breathlessness.
Here is an important warning applied to Midazolam courtesy of the US National Library of Medicine:
“Midazolam injection may cause serious or life-threatening breathing problems such as shallow, slowed, or temporarily stopped breathing that may lead to permanent brain injury or death. You should only receive this medication in a hospital or doctor’s office that has the equipment that is needed to monitor your heart and lungs and to provide life-saving medical treatment quickly if your breathing slows or stops. Your doctor or nurse will watch you closely after you receive this medication to make sure that you are breathing properly.”
The warning states that this medication should only be given in a hospital or doctor’s office that has the necessary equipment to monitor the patient’s heart and lungs and provide life-saving treatment if needed.
The question is therefore raised as to why the “Death Document” published in April 2020 instructs doctors to treat covid-19 patients suffering a disease that allegedly affects the respiratory system with Midazolam, a drug that affects the respiratory system.
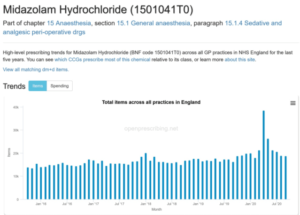
Another question is raised as to why during the same month out-of-hospital prescribing for Midazolam was twice the amount seen in 2019.
This raises concerns about the appropriateness of the treatment being given to covid-19 patients in care homes during the pandemic.
The CQC, a statutory body commissioned by the Department for Health and Social Care, conducted a special review of Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) decisions made during the covid-19 pandemic. The investigation found evidence of unacceptable and inappropriate DNACPR’s being made throughout the pandemic and states that it is possible that cases of inappropriate DNACPR’s remain in place.
The CQC’s investigation also found that throughout the “pandemic” this guidance was not being followed as they had received deeply troubling evidence from numerous sources that during the covid pandemic DNACPR notices have been applied in a blanket fashion to some categories of person by some care providers, without any involvement of the individuals or their families.
Almost 10% of people using services or families who responded to their call for evidence told the British Institute of Human Rights that they had experienced pressure or use of DNACPR orders.
Thirty-four per cent of people working in health and/or social care said they were under pressure to put DNACPR’s in place without involving the person.
In addition, 71% of advocacy organizations and campaigners said they experienced DNACPR orders put in place or pressure to make them without being involved in the decision.
It’s also noted that these DNACPR orders were wrongly used as an excuse to begin end-of-life care.
The Death Document
NICE claims to be an independent organisation but in truth it seems to be anything but once you look into its structure. On this page here you will see the quote “Our Structure – The structure of the organisation and how we work with the government”. Following the link to the “Our Structure” page here, and then clicking “Find out more about how we develop guidelines” takes you to a page here from which is it clearly stated that “Topics are referred to NICE from the following organisations”:
- Healthcare topics: NHS England
- Public health topics: Department of Health and Social Care
- Social care topics: Department of Health and Social Care and Department for Education.
A copy of the NICE framework is here which you can go through at your leisure. As you will see at Clause 4.1 “The Secretary of State is accountable to Parliament for the health system (its ‘steward’), including NICE”.
All the above information points to NICE not being independent at all. It is clearly part of the UK government, (NICE is funded by and accountable to the Department of Health and Social Care) and operates as an agency of the NHS. Further, and worryingly, given that it does not appear to be an independent organisation, the reach of NICE is extremely wide ranging given their guidance is implemented not only in hospitals, but in GP practices, and care homes and community organisations, along with others, and extends internationally.
Therefore, we need to ask the question “Are the UK government, via the Department of Health and Social Care, responsible in any way for NICE guideline NG163 which led to the unnecessary killing of the UK’s elderly and most vulnerable by recommending the use of Midazolam and Opioids for the ‘treatment’ of covid 19?”
This document is tricky to find. If you search for it on the NICE website, you will reach a page that states that this guidance has been updated by NG191, which supersedes it. There is no library copy of NG163 for you to look at.
Clare Wills Harrison, a lawyer who has been exposing the Midazolam scandal since 2020, found NG163 some time ago along with multiple other documents which have since come to light and are relevant to the Midazolam issue. It is fair to say that NG163 has directly led to the incorrect use of a protocol which Clare and her team call “the death pathway”, and they have come to the conclusion that where the word “pathway” appears in any medical recommendations, this is normally a cause for concern.
You can read NG163 yourself by clicking here.
When you read NG163, note the date – 3rd April 2020. This was less than 2 weeks after the UK entered lock down. Even if we concede that NICE, via the government, were working on treatment guidelines from January 2020, when early reports of covid 19 were circulating around the world, that would have given NICE only 3 months to formulate the guidance in NG163. It is inconceivable that NICE could have the evidence and effectiveness information about the use of Midazolam and Opioids for the treatment of breathlessness and anxiety in covid 19, within this time frame.
NG163 clearly states, Midazolam did not have a UK marketing licence to be used for breathlessness or agitation at the date of its publication. If prescribed for the same, it would therefore be regarded as being used off label. A PowerPoint presentation created by Clare Wills Harrison (see here) explains the extra requirements placed on anyone prescribing a medicine off label. You should also consider the consistent refusal by the UK health agencies to allow prescribing off label for other cheap anti-viral drugs to treat covid.
The GMC regulates doctors in the United Kingdom. They set standards, hold a register, quality assure education and investigate complaints.
On 14th April the GMC put out a “Joint statement: Community-based prescribing for covid-19 symptoms” which you can find here.
The joint statement irrefutably supports the NICE guidance in NG163 –

It’s quite clear, from the evidence provided by whistleblowing NHS staff, investigative lawyers, and official Government reports is that you gave up over two years of your life due to a lie.
A lie that involved prematurely ending the lives of thousands upon thousands of people, who you were told died of covid-19.
A lie that has involved committing one of the greatest crimes against humanity in living memory.
A lie that has required three elements: fear, your compliance, and a drug known as Midazolam.
yogaesoteric
May 24, 2023