The ‘Disappearance’ of Polio (II)
A story about how to vaccinate people against a friendly pathogen which helps humans to acquire natural immunity, and about vaccine production and vaccine approval despite harmful effects
The following article is a series of extracts from Dr. Suzanne Humphries’ book Dissolving Illusions.
Read the first part of the article
If polio is still here, why don’t we see it?
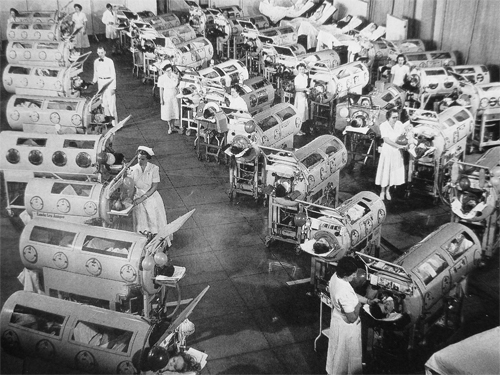
Wild poliovirus was never the big killer or paralyzer the public was led to believe it was through the many frightening images shown repeatedly in the 1950s. Dr. Lennette, a well-respected virologist and pioneer of diagnostic virology with the California Department of Health, said in reflection on September 1987: “Actually, economically the disease wasn’t very important. Secondly, not many cases were seen in this country. There weren’t too many people paralyzed from polio in any one neighborhood, so it never made much of an impact.” (See also Graph 12.1 from the first part of this article.)

The pictographic and cinematic images of polio that were used to rally the public toward vaccine development and acceptance dropped away after the vaccine campaign began. The public gratefully embraced the vaccine that was believed to have removed the frightful disease. To maintain public belief in the vaccine, especially in light of several serious instances of vaccine-induced paralytic polio, the images of polio in the new, highly vaccinated population had to be deleted.
Optimism regarding the vaccine prevailed. The March of Dimes campaigns that were once designed to impact human fear and emotion transitioned into what we see today as advertising for “working together for stronger, healthier babies” – funding vaccines for infants and pregnant mothers.
Today, in Gaza, India, and Nigeria, where poliomyelitis is prevalent and limbs are treated according to the old ways, outcomes are similar to the images of the 1930s and 1940s. Those images of crying children in plaster casts, used to influence the population to accept vaccination, were quite rare when the Kenny method was used. How welcome would polio vaccine campaigns be today, if Sister Kenny’s method (Sister Elizabeth Kenny was a nurse from the Australian outback whose observations led her to treat polio with hot packs and physical therapy) was implemented in Gaza, India, and Nigeria and those unnecessarily deformed and atrophied limbs were nonexistent?
Pesticides
By the 1960s, there was convincing evidence that polio-virus could live quite happily in pesticide-treated cells, and more over, that the pesticides led to increased susceptibility of viral invasion. DDT was found to enhance the release and intracellular multiplication of poliovirus. Thus, it likely contributed to creating a monster out of a normally benign gut virus. Unfortunately, this information was not published in the medical literature until a full decade after the polio vaccine was an accepted solution to poliomyelitis. Coincidentally, DDT was phased out of use in the United States and Canada beginning in the 1960s, right around the time that polio was disappearing.
Diet
During summer months at the beach, sugared foods were consumed in large volume. Sugar is known to create a toxic environment in the gut, altering the balance of beneficial and toxin-producing bacteria. Together with DDT, sugar would have created the perfect storm to damage the bowel and systemic immune systems.
Diet, in particular diets high in refined sugar and flour, has a known impact on susceptibility to severe poliovirus infection. The harsh chemicals used in cane sugar refining are thought by some scientists to have contributed to the synergy between an otherwise innocent virus and the sugar. In addition, as Dr. Sandler demonstrated, sugar metabolism and post-prandial hypoglycemia increased cellular viral susceptibility.
Toxins
The paralysis that the world witnessed in the first part of the 20th century was largely from toxins in the environment like DDT, lead, and arsenic. Those toxins seriously disrupt mucosal immunity, allowing a previously benign virus to bypass the innate immune system and cause paralysis and other clinical symptoms. Where those chemicals are still used today, you will see reports of paralysis, which used to be called “polio”, but authorities now call it “acute flaccid paralysis.”
This following diagram reveals the parallel between polio epidemics in the United States and tonnage of pesticide (most of which was DDT) production from 1940 to 1970.
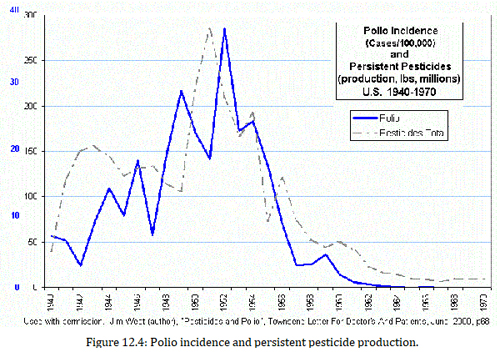
It’s no small wonder that polio appeared to be such a vicious entity from the late 1800s and up until DDT was phased out of use in the United States. But that didn’t happen until after a vaccine for polio was fully embraced as a savior of humanity in 1954. The United States was considered free of wild polio as of 1979.
Today in India, “polio” is a well-publicized problem, and DDT can be found on shelves just about anywhere. India, one of four countries that still manufactures DDT, remains the chemical’s largest consumer and producer.
China suffered an epidemic of polio in 2011 and is one of the four countries that has produced and continues to use DDT.
Although breast milk DDT levels in women in the United States is among the lowest in the world after decades of its banning, many other countries are still polluted with the chemical.
Morbidity of polio, then and now
The CDC defines polio’s statistical paralytic rate and estimates that it is less than 1 in 100 for some sort of permanent paralytic syndrome. “Approximately 95% of persons infected with polio will have no symptoms. About 4-8% of infected persons have minor symptoms, such as fever, fatigue, nausea, headache, flu-like symptoms, stiffness in the neck and back, and pain in the limbs, which often resolve completely. Fewer than 1% of polio cases result in permanent paralysis of the limbs (usually the legs). Of those paralyzed, 5-10% [of that 1%] die when the paralysis strikes the respiratory muscles.”
Prior to vaccination, Dr. Maurice Brodie reported that only 1 in 170 children with no antibody to polio became ill during epidemics. By these two drastically different risk estimations, you can see that statistics are not set in stone, nor are they necessarily a reliable indicator of risk. The CDC reports a 59% higher paralysis rate (after vaccination) than was actually measured during a pre-vaccine epidemic.
The question to ask today is, how much poisoning by chemicals and infection with other viruses was counted as polio in the statistics? According to the CDC, less than 1 percent of infected people develop paralysis, and 5-10% of that 1% suffer respiratory death. Yet in several polio epidemics, far more than 1 percent were paralyzed and even died.
Laboratory and vaccine sources of epidemics
Nowhere else in polio’s history was there more panic than during New York City’s 1916 epidemic. Dr. H. V. Wyatt published a document in 2011 discussing the possibility that a highly virulent laboratory-engineered strain of poliovirus “escaped” from the Rockefeller laboratories, causing the largest epidemic of polio in US history. Just what exactly could have escaped from the lab is unknown. At the time, the epidemic was broadcast to the public as having been started by children who arrived from Italy. But the immigration data does not fit with that hypothesis. Official immigration books show that the epidemic began before those children arrived.
The epidemic was unique in that the virus was highly destructive to the nervous system, much like the Rockefeller labs cultivated “MV” strain. “Three miles from the epicentre of the outbreak, Simon Flexner and his associates at the Rockefeller Institute at 63rd Street and York Avenue, near Queensborough Bridge on Manhattan Island, had been passaging spinal cord tissue containing poliovirus, from one Rhesus monkey spinal cord to another. These experiments continued with the passage virus which at times was reinforced with newly acquired virus from patients … Those doctors had no awareness of what they were handling… By 1916, mutants of the original Rockefeller virus had been selected for replication in monkey motor neurones, but were still capable of high levels of replication in other cells… It is a remarkable coincidence that a unique neurotropic strain of poliovirus was developed a few miles from an epidemic caused by a uniquely pathogenic strain of the virus… A few blocks from the Rockefeller Institute at Lexington Avenue and 63rd Street the 3rd Avenue elevated line linked at Municipal Building station to the BRT line to Brooklyn over Brooklyn Bridge with a stop at 3rd Street and 5th Avenue where the first case lived. However, almost anywhere in New York was within a few streets of a rail link to the Rockefeller Institute.”
The significance of this epidemic is that it set the stage for the terror to come. Doctors and parents alike, after this aberrantly lethal polio epidemic, were perched for an ominous future and thus ready and willing to do whatever was necessary to eradicate polio.
Many doctors of the 1940s were aware that the pitchmen of the National Foundation for Infantile Paralysis (NFIP) and March of Dimes were responsible for the expanded terror that swept the nation. Few today are aware of the intimate relationship between the NFIP and the Rockefeller Institute. Nearly all the researchers for the polio vaccine were from Rockefeller. Dr. Thomas Rivers, virologist and director, was an “unpaid consultant” to NFIP and Basil O’Connor (NFIP’s founder) and also served as mentor and advisor to Albert Sabin and Thomas Francis.
Sabin developed the live vaccine that is now used in India, and Francis headed the largest public health experiment in history, the Salk vaccine trial of 1954. Rivers was the commandant of the plan to conquer polio in 1938. He is rumored to have had a serious distaste for Sister Kenny, as did AMA’s Morris Fishbein and NFIP’s Basil O’Connor. NFIP’s attempts to buy her and discredit her were, fortunately, futile.
Synthetic poliovirus
Today, laboratory generation of infectious virus in the absence of a natural viral template has been accomplished by scientists. It was funded by the US Defense Advanced Research Project Agency (DARPA). Dr. Eckhard Wimmer, one of the scientists involved in the project, reported: “The empirical formula of poliovirus is C332,652H492,388N98,-245O131,196P7,501S2,340 … Placing the atoms in order, a particle of high symmetry emerges… Our experiment has thus overthrown one axiom in biology – namely, that the proliferation of cells or, for that matter, viruses depends on the physical presence of a functional genome to instruct the replication process. It was believed that without parental genomes, no daughter cells or progeny viruses would arise. We have broken this fundamental law of biology by reducing poliovirus to a chemical entity, which can be synthesized on the basis of information stored in the public domain…. Just like a common chemical, poliovirus has been synthesized in the test tube.”
Dr. Wimmer also reports that neurovirulence can be manipulated readily in synthetic polioviruses, though he presumes that this capability will be used for attenuation rather than for raising more virulent species. Either one is equally possible.
The Cutter disaster and other vaccine blunders
Most people today don’t know about the infamous Cutter disaster. This was a virus-related poliomyelitis epidemic that was initiated by the use of the Salk vaccines just after they were rapidly developed and fast-tracked into licensure by the US Department of Health, Education, and Welfare. This record-breaking approval process took only two hours.
Because of outside pressure, the licensing committee in charge of approving the vaccine did so after deliberating but without first having read the full research, namely the Francis Report on which their approval was to have been based. Dr. Howard Shaughnessy, laboratory director, Illinois Department of Health, testified to this event: “Previously it [the vaccine] had been distributed as an experimental product, not a licensed product … the committee was asked to come to a decision very quickly … there was discussion of the report that Dr. Francis had given, but we were not in a position to discuss it very intensively because we had not seen the report prior to this morning and the report was distributed to us after the presentation … we were pressured in the sense that we were told that speed was essential, and when we came up toward the 5:00 time, some of us felt we would like to discuss this matter more. We were told that to discuss the matter further it would have to go into the following week, and we would have to go to Washington or Bethesda and most of the members were unwilling to do so. We were in effect pressured into an earlier decision than we ordinarily would have made… It was part of the pressure of events, put it that way.”
Dr. Thomas Francis did not issue the final report of his evaluation of the 1954 field trials until April 1957, two years after the licensing of the vaccine. At the time, public health authorities decreed that physicians inject the fast-tracked vaccine before those doctors knew much about the science or the large Francis trial. The consequences of this impulsive action turned out to be significant.
The Salk invention was an injectable, supposedly formaldehyde-inactivated version of poliovirus vaccine. There were serious problems with the viral inactivation process that were known by insiders from the outset of the vaccine’s development. Any professional objection by scientists involved during the development of the vaccine was rapidly subdued. Dr. Paul Meier attested to the practice of firing scientists who disagreed with the NFIP’s plans. “Jonas Salk had a paper in which he argued that all the virus was inactivated, and that there was no live virus left. But, the sixth lot was not listed. And so I said that something was wrong. He cut out data in order not to show what happened to some lot…. Well, NFIP did form an advisory committee. And they reformed it five or six times. Each time somebody didn’t agree, they dropped them and got somebody who might agree. By the time they were done forming the committee, everybody on it was distinguished, but very agreeable.”

As a result of ignoring the warnings by highly qualified scientists who repeatedly and publicly explained why and how the inactivation process was flawed from the beginning, the vaccine virus needlessly infected, paralyzed, and killed children and their household contacts. “Others Wendell Stanley, Sven Card, Enders, Herdis von Magnus and myself among others disagreed, convinced that the inactivation process did not follow a straight line and it was not permissible to extend the curve below the baseline… And I remember Colin MacLeod raising the question whether this was really the way to go, but that’s the way the matter stood, namely, ‘We’ll go ahead and make the vaccine.’ Well, the vaccine was made that way. Then Cutter made several batches of the vaccine, which upon inoculation into man produced cases of poliomyelitis, some of them with severe paralysis.”
Millionaire vaccine inventor Paul Offit, a supporter of mandatory vaccinations, wrote a book on the Cutter incident. In the book, even he admits: “… the disease caused by Cutter’s vaccine was worse than the disease caused by natural polio virus.”
There is a body of literature that speaks to the real cause of the problem, which was known from the outset of the development of Salk’s vaccine.
Dr. Thomas Rivers, the mastermind of Rockefeller’s polio vaccine mission, hired all the chairmen of departments of virology. He had enormous clout, and nobody dared argue with him, lest their careers be ruined.
Dr. Lennette, talking about a pre-vaccine trial meeting of the minds in New York City in 1953, said: “Tom Rivers was there, Tommy Francis, Joe Smadel, and Colin MacLeod, all of whom were deeply involved. These were people to whom you might apply the term ‘the establishment,’ … These were the ‘old graybeards’ who had been through the mill of medical science … The question was raised as to whether the vaccine would be safe at the present level of inactivation with formaldehyde. And I remember distinctly Tom Rivers saying, ‘If you put any more formaldehyde in, you’ll make it so damn safe it won’t be any good.’ That’s recorded somewhere in the minutes of that meeting.”
Salk and the scientists who remained on the NFIP board interpreted the formaldehyde inactivation curve incorrectly. As a result, live virus remained.
There was yet another factor in the virulence of the 1955 vaccine. The vaccine used in the 1954 trial contained Merthiolate, a mercury compound that had a virucidal (virus-killing action) effect. Because Jonas Salk was disappointed in the antibody-stimulating effect that the 1954 field trial demonstrated, the Merthiolate was removed in the 1955 vaccine to induce a faster antibody response in vaccine recipients. Not only was the 1955 vaccine not the same celebrated vaccine that was trialed in 1954, it was also riddled with live viruses of a highly neurovirulent nature – the Mahoney strain.
Between April 17 and June 30, 1955, 260 poliomyelitis cases were documented after inoculation of about 400,000 persons with the Cutter vaccine. Ninety-four cases were among vaccinees, 126 among family contacts, and 40 among community contacts. An estimate of the case-infection ratio is in the range of 1 case per 100 to 600 injected infections.
It is a documented fact that household adult contacts did contract polio, secondarily, from the vaccine, and some became severely paralyzed. Thirteen household contacts required iron lungs, and five died. There were documented cases where infants received the vaccine injection, shed live virulent virus in the stool, and never got sick. But their mothers became very ill, and so did neighbors. A conservative report revealed that 39 friends and neighbors of children who received the Cutter vaccine were paralyzed. Many more were infected to lesser degrees.
The newly formed Polio Surveillance Unit (PSU) did not capture all the cases that developed from the domino effect of this grand mishap. The reason is that they had strict cutoff dates beyond which any reported polio was considered not to be from the vaccine.
Paul Offit summarized the estimate of known damage: “In the end, at least 220,000 people were infected with live polio virus contained in Cutter’s vaccine; 70,000 developed muscle weakness, 164 were severely paralyzed, 10 were killed. Seventy five percent of Cutter’s victims were paralyzed for the rest of their lives.”