Warning – Are You Being Targeted For Euthanasia?
By Mary Therese Helmueller
(U.S. Registered Nurse)

In 1984, while working as charge nurse in the intensive care unit, a 20-year-old man asked me: “Can you give my mother enough morphine to let her sleep away?” I was horrified. “I cannot kill your mother”, I responded. That was only the beginning. Recently, an 80-year-old was admitted to the emergency room and the physician said: “Let’s dehydrate her”; one more patient was sentenced to die in hospice with no terminal diagnosis and once again, the living will determined the death of a 70-year-old man regardless of how he pleaded to live. I can no longer remain silent.
Your life may be in danger if you are admitted to a hospital, especially if you are over 65 or have a chronic illness or a disability. The elderly are frequently dying three days after being admitted to the hospital. Some attribute it to “old age syndrome” while others admit that overdosing is all too common. Euthanasia is legal in certain US states, and it is being practiced. The New England Journal of Medicine reported that 1 in 5 critical care nurses admit to having hastened the death of the terminally ill! I believe the percentage is much higher. I have worked with nurses who even admit to overdosing their parents. No one knows the exact euthanasia rate in the United States, however Dr. Dolan from the University of Minnesota states that 40 percent of all reported deaths is probably a conservative estimation. If this is true, then the United States is executing euthanasia at a higher percentage rate than the Netherlands, where it is also legal and widely practiced.
Did you know that many doctors and nurses whom we trust are speaking openly about their desire to practice euthanasia? In fact, they are even speaking about ending their own lives when they reach the age of 65 or before if diagnosed with an illness. Some even admit to stealing the drugs for their own lethal injection. Think about it. These are the same people who will determine the value of your life. If they do not value their own, how can you expect them to value yours?
I am a registered nurse in the St. Paul/ Minneapolis area with 15 years experience in emergency and critical care. My knowledge of euthanasia not only comes from my experience working in the critical care units throughout the Twin Cities, but also comes from a personal tragedy and loss in 1995. This is my true story. My hope is that you will educate others and protect yourselves and loved ones.
On Monday, February 20th, my grandmother was admitted to a local Catholic hospital with a fracture above the left knee. She was alert and orientated upon admission but became unresponsive after 48 hours and was transferred to hospice on the fourth day, and died upon arrival.
I was in Mexico City conducting a pilgrimage and unable to be at her side so there were many questions upon my return. The doctors could not tell me the cause of her death, so I began to search for the answers and was fortunate to obtain the hospital chart. It then became very clear that my grandmother had been targeted for euthanasia!
Carefully tracing the events it was evident that my grandmother became lethargic and unresponsive after each pain medication. She would awaken between times saying: “I don’t want to die, I want to live to see Johnny ordained”, “I want to see Greta walk”. Johnny was her grandson studying in Rome to be a priest and Greta was her new great-grandchild. Even though over-sedation is one of the most common problems with the elderly, she was immediately diagnosed as having a stroke. When she became comatose, a completely hopeless picture of recovery was portrayed by the nurses and doctors who reported that she had a stroke, was having seizures, going in and out of a coma, and was in renal failure.
The truth, however, can be found in the hospital chart which indicates that everything was normal! The CAT scan was negative for stroke or obstruction, the EEG states “no seizure activity” and all blood work was normal indicating that she was not in renal failure! How were we to know that the coma was drug induced and that all the tests were normal? Why would they lie?
Looking over the chart it is clear that obtaining a “no code” status was the next essential step in executing her death. This is an order denying medical intervention in emergency situations. The “no code” was aggressively sought by the medical profession from the moment of her admission but was not granted by my family until it appeared that she was dying and there was no hope. Minutes after obtaining the “no code”, a lethal dose of Dilantin (an anti-seizure medication) was administered intravenously over an 18-hour period. It put her into a deeper coma, slowing the respiratory rate and compromising the cardiovascular system leading to severe hemodynamic instability. The following day she was transferred to hospice and died upon arrival. The death certificate reads “Death by natural causes”.
My grandmother had no terminal diagnosis but the hospice admitting record indicates two doctors signed their name stating that she was terminally ill and would die within six months. How was this determined? The first doctor, who was the director of hospice, never came to evaluate her or even read the chart. More interesting is the fact that the second doctor was on vacation and returned three days after her death! Obviously these signatures were not obtained before or even upon her admission to hospice. How can this be professionally, morally or even legally acceptable? Can anyone therefore be admitted to hospice to die? It certainly seems possible especially if sedated or unresponsive. In fact, this hospice has recently been under investigation for accepting hundreds of patients who had no terminal illness.
It Could Happen To You
How can this happen? A serious problem lies in the definition and interpretation of “terminal illness” which permits the inclusion of chronic illnesses and disabilities. Terminal illness is defined as “an incurable or irreversible illness which produces death within six months”. The fact is that many chronic illnesses such as diabetes and high blood pressure are incurable and irreversible and without medical treatment such as insulin and other medications these illnesses would also produce death within six months. Therefore, those with chronic illnesses or disabilities can be conveniently denied medical treatment and even food and water to make them terminal. Typically it is the elderly who arrive in the hospital that are at the greatest risk. But it could be anyone! Especially those whose life and suffering is viewed as useless and burdensome.
Difficult to believe? Well it was for our prolife lawyer until his mother-in-law was admitted to a hospital several months later for a stroke. She became “unresponsive” and “comatose” a few days after her admission. The neurologist wrote an order to transfer her to hospice refusing an I.V. and tube feeding staring “this is the most compassionate treatment”. Remembering my story, our lawyer requested the removal of all narcotics and demanded an I.V. and tube feeding. This infuriated the neurologist. He began to accuse the family of being uncompassionate and inhumane. To prove his point he began a neurological assessment on the patient. Just then she opened her eyes and pulling the physician’s necktie, forced his face to hers and said very clearly “Give me some water!” It was obvious that she was awake, alert and orientated. He angrily cancelled the transfer to hospice and ordered a tube feeding and intravenous. Several weeks later she was discharged and was exercising on the treadmill! She escaped the death sentence. Unfortunately many others like my grandmother have not. A stroke does not make you terminal, but not receiving food and water does!
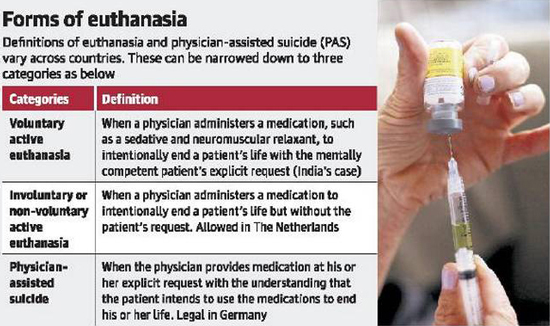
A clear understanding and definition of euthanasia is essential for a correct and moral judgment. Unfortunately the meaning is being altered by those who hold society’s values and by those who seek financial gain. According to the Congregation for the Doctrine of the Faith and reaffirmed by Pope John Paul II in his encyclical letter Evangelium Vitae euthanasia is defined as “an action or omission which of itself and by intention causes death, with the purpose of eliminating all suffering”.
The killing in hospitals today is commonly referred to as “the exit treatment” and disguised by the word “compassion”. Many doctors and nurses honestly believe that this is the most compassionate treatment for the elderly, the chronic and terminally ill, especially those whose suffering is seen as hopeless, inconvenient and a waste of time or money. Those who hold this twisted and corrupted idea of compassion actually believe they are doing good because suffering has no value and materialism is their god. For instance, how often have we heard that Medicare and Medicaid are “running out”? “So why not relieve pain and lighten the financial burden of our families and society”?
As a result, many patients are intentionally over sedated and forced to die from dehydration, starvation or over medication. “Death by natural causes” will be officially documented on the death certificate. Did you know that this is the exact same proclamation on the death certificate of St. Maximillian Kolbe? Everyone knows however that he died from a lethal injection in Auschwitz concentration camp after many days of dehydration and starvation!
Pope John Paul II states clearly in his encyclical Evangelium Vitae: “Here we are faced with one of the more alarming symptoms of the ‘Culture of Death’ which is advancing above all in prosperous societies, marked by an attitude of excessive preoccupation with efficiency and which sees the growing number of elderly and disabled as intolerable and too burdensome”.
Many souls are being denied the opportunity to reconcile with God and family members because their death has been hastened or deliberately taken. This is a grave and moral injustice. Pope Pius XII in his Address to an International Group of Physicians on February 24, 1957 stated: “It is not right to deprive the dying person of consciousness without a serious reason”. Pope John Paul II confirmed this in Evangelium Vitae saying: “as they approach death people ought to be able to satisfy their moral and family duties, and above all they ought to be able to prepare in a fully conscious way for their definitive meeting with God”.
Recently the Carmelite Sisters shared this tragic story of a friend whose husband was euthanized. Her husband was diagnosed with terminal cancer but was not expected to die for several months to a year. He had been away from the Catholic Church and the sacraments. He also was estranged from his children. One day he complained of pain that was not relieved by medication. The wife spoke to the nurse who then called the doctor. When the doctor arrived he gave an injection through the intravenous line. The husband took three breaths and died! The wife screamed: “I did not ask you to kill my husband!”
“We needed time to reconcile our marriage and family!” She continued to cry: “He needed time to reconcile with God and the Church!”
It is evident that euthanasia is being even more cleverly planned and executed. A priest from St. Paul was called to the hospital by a nurse to administer the last sacraments to a hospice patient. When the priest arrived he was surprised to find the patient sitting up in the chair! He visited with the patient approximately a half hour then heard his confession and administered the last sacraments. Just before he left the room the patient jumped up in bed and the nurse administered an injection. Perplexed and concerned, the priest called the hospital upon returning to the rectory. The patient had already expired!
There is a good and legitimate purpose for hospice units, but how can it ever be morally acceptable to transfer patients to a unit to die when they have no terminal illness? How can sedating a patient and refusing a tube feeding and intravenous be considered compassionate? Dehydration and starvation is not a painless death! Has this become the Auschwitz of today? A convenient and economically efficient place to dump the unwanted, imperfect, and burdensome of our society?
Would a “living will” prevent these tragic events? The living will makes you a clear and easy target to be euthanized. A “living will” has nothing to do with living. It is your death warrant. It actually gives permission to facilitate your death by denying medical treatment. Did you know that it was originally developed by Luis Kutner in 1967 for the Euthanasia Society of America? It is the most cost effective tool for hospitals, insurance companies, Medicare and Medicaid. Therefore, since 1990 it has been deceptively packaged and promoted as a patient’s right known as “the Patient Self-determination Act”. If cutting care for those patients who ask for it wasn’t so successful in saving money and controlling the budget, why then did it originate in the Senate Finance Committee and why was it supported by the House Ways and Means Subcommittee on Health? These are finance committees whose only interest is controlling the budget! It is obvious that the living will is all about saving money, not your life!
Many people fear the loss of control that comes with illness and hospitalization. Tragically, they are deceived in thinking that the “living will” protects them and restores this control in their lives. Nothing could be further from the truth. No one knows the exact condition in which they will be admitted to the hospital. The “living will” is written in very broad terms leaving it open to the interpretation of medical professionals and others who stand to benefit from your demise. Remember your best interests or your interpretation may not be theirs! Can you imagine writing general instructions or signing a legal contract for the care of your Mercedes Benz several years before any problem occurs? “Please do not give oil or gas”; “If in three days it cannot be fixed stop everything and trash the car”. How absurd and ridiculous! It takes time to diagnose and treat even car problems! If we would not foolishly demand this for a car then how can we demand it for a human life which has an eternal value?
Recently, a 70-year-old was admitted through the emergency room in respiratory distress. He was placed on a ventilator and transported to the intensive care unit. He was awake, alert and orientated anxiously writing notes: “I don’t want to die”, “I changed my mind”, and “Please don’t take me off the machine”. He was very persistent and urgent with his pleading. I soon understood why! His family and physicians were meeting to discuss a serious problem. He had signed a “living will” declaring that he did not want “any extraordinary measures”. He was now viewed as “incapable” of making any decisions and they wanted to follow his wishes as stated in the legal document! Very convenient for those who do not want their inheritance spent on hospital costs and for those who do not want to be bothered with a “useless burden” to our society!
Today hospitals and health care facilities are required to ask patients if they have a living will or lose government funding! The question is proposed in such a way to create pressure on patients so that they think it is something good, desirable and necessary. “Do you know that you have a right in the state of Minnesota to possess a living will?” Please remember that the living will targets you for euthanasia by denying you medical treatment. Living wills kill: they do not protect you. Instead, I urge you to obtain a copy of “The Protective Medical Decisions Document” (PMDD) from the International Anti-Euthanasia Task Force, www.internationaltaskforce.org P.O. Box 756, Steubenville, Ohio 43952. U. S. Phone no: 740-282-3810. Sign it and keep it among your records. Please get rid of your living will!

Can you or a loved one be targeted for euthanasia without a living will? The course of events and treatment in my grandmother’s short hospitalization are documented. She did not have a living will. Please know the following steps – it could save your loved one’s life.
1. Over sedation Causing Lethargy And Unresponsiveness Difficulty or inability to awaken a patient.
Some patients, especially the elderly, are very sensitive to pain medications which are slowly metabolized by the liver. Toxic levels build quickly with very small doses commonly producing lethargy and unresponsiveness. Elderly patients require approximately 20% less of the normal adult doses.
2. A Hopeless Picture Of Any Recovery the patient appears to be comatose and dying. The medical staff affirms this with overwhelming reports and statements.
3. No Code Status Also Referred To As DNR/DNI (do not resuscitate/ do not intubate). The consent is obtained from the family. It is a request to deny a patient delivered emergency care in a life-threatening situation.
4. Lethal Doses Of Dilantin Or Narcotics (morphine). This will hasten the death, shortening the hospital stay and expenses.
5. Transfer To Hospice Without Tube Feeding Or Intravenous due to sedation and inability to eat or drink the patient will die of dehydration and starvation.
If a loved one is lethargic or unresponsive demand to see the medical chart and medications sheet. If you do not understand the terminology and medications, consult a pharmacist. A computer printout is available at pharmacies on most medications. If you suspect over sedation speak to a prolife doctor or nurse and then ask to stop all narcotics and wait at least for 48 hours to see if there is any improvement. Contact prolife organizations such as National Right to Life Committee to obtain information and local phone numbers of prolife organizations, doctors, nurses or lawyers in your area: National Right to Life Committee: http://www.nrlc.org/default.html, 512 10th St NW Washington, D.C. 20004; 202-626-8820.
Think twice before giving consent to a “no code status”. It has become too convenient for those nurses and doctors who hasten the death of their patients! Furthermore, it not only denies emergency medical treatment but many professionals also deny the following: antibiotics for pneumonia, medications and assistance to choking victims!
If your loved one is being transferred to hospice do not assume there is a terminal illness. Ask to see the chart especially in regards to unresponsive elderly and comatose patients. Remember that “comatose” is not a terminal illness, but not receiving food and water will make anyone terminal! Always ask for a second opinion. Consult with prolife nurses or doctors.
If you need assistance in finding a prolife doctor, information, or just need to discuss your concerns on a particular case, please contact The Moscati Institute; 2901 Branch Street: Duluth MN 55812 Ph: 218-728-4608.
Your life may be in danger especially if you are over 65 and admitted to the hospital. Euthanasia is legal in the United States and is being practiced. Recently, Dr. Kevorkian in a TV interview said: “Why is everyone focused on me? There are many more doctors doing the same thing!” A pediatric cardiologist who interviews students for a prominent medical school on the east coast recently reported that more than 95 percent agreed with Dr. Kevorkian’s practices. The culture of death has permeated the minds of our doctors before they enter medical school! Obviously euthanasia is already being taught through the media, entertainment, primary and secondary schools and even in our families!
Euthanasia is embraced by the lack of values in our society. It is the result of a culture that has accepted and promoted the killing of unborn children. The value of life is the extent of the pleasure and wellbeing it brings. Suffering, imperfection, illness, and inefficiency are viewed as unbearable setbacks, useless and burdensome. Death is viewed as a “rightful liberation”. As a result, euthanasia is packaged to appear desirable and then sold to the unsuspecting public as the “living will”, “death with dignity” and “the right to die”. Is it not logical that those who can kill the child in the womb will also kill their parents in their old age for the same reasons of convenience, so-called “compassion”, money etc.?
We should think twice about promoting euthanasia by saying: “I hope there is a Kevorkian around when I get older”, or “Just shoot me if I ever become like that”. There is a great spiritual value to suffering. Every human life must be valued and supported as a precious gift. We cannot afford to patronize movies, TV programs, businesses or any forms of entertainment that promote, encourage and support the killing of innocent life. Prolife political candidates deserve our support and votes. It is imperative to be informed. We cannot fight what we do not know or do not see. You can contact Human Life International and ask for their monthly newsletter. Human Life International; 4 Family Life; Front Royal, VA 22630; phone: 540-635-7884: FAX: 540-636-7363.
More importantly, we must work to convince government officials and medical professionals to protect all human life from the moment of conception to natural death. You have escaped death by abortion, but you are all being targeted for euthanasia!
yogaesoteric
November 2, 2018