What We’ve Learned from a Year of Vaccine Shedding Data (3)
Read the second part of the article

Circulatory Symptoms
In addition to the neurological symptoms, other circulatory issues were also reported:
- The heart issues were primarily chest pain, angina and tightness,1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 atrial fibrillation,1 2 3 4 5 6 7 8 9 10 11 12 along with heart palpitations, arrhythmias, tachycardia or PVCs.1 2 3 4. 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47
- A few heart attacks,1 2 3 4 5 myocarditis1 2 3 4 5 (including a fatal case and myocarditis following blood transfusion), pericarditis,1 2 pericardial effusion, cardiomegaly, possible heart failure, pre-existing cardiomyopathy worsening.
- Severe blood clots,1 2 3 4 5 6 7 8 9 10 11 12 some of which were life threatening (e.g., pulmonary embolisms) and resembled those seen after the vaccine. Additionally, clots were reported in one cat and many minor clots have been observed as well.1 2 3
- Raynaud’s,1 2 3 4 5 peripheral arterial disease, lumps on blood vessels, and an acupuncturist reporting that her limbs, abdomen and veins will consistently turn blue 4-6 hours after working with triple-vaccinated patients.
- A hypertensive emergency and elevated blood pressure.
Note: May-Thurner syndrome (for 2 months) and symptoms suggestive of erythromelalgia or venous insufficiency (e.g., feeling like one’s blood was on fire, severe insomnia, extreme cold and cold aversion, sun sensitivity, swollen red and dry looking veins) were also reported.
Immune Suppression
Additionally, a subset of readers appeared to develop immune suppression due to shedding.
As shingles is one of the most common illnesses triggered by immune suppression, it has also been the most common one triggered by vaccination and shedding.1 2 3 4.5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55
Activations of herpes,1 2 3 4 5 6 7 Lyme disease,1 2 3 4 5 6 7 Epstein Barr1 2 3 4 5 6 7 8 9 have also been repeatedly reported.
Note: reactivations of Epstein Barr and herpes have been repeatedly observed in covid vaccine injured patients.
Many patients have reported a chronic susceptibility to illness after vaccination1 2 3 4 5 6 7 8 9 10 (including in a child and one case where serial lab work showed shedding repeatedly caused immune suppression).
Lethal pneumonia, near lethal pneumonia through secondary shedding, bronchopneumonia, and unusual bacterial infections occurred as well.
Note: lastly, an oral mucocele (blood blister), cherry angiomas, styes and eyelid swelling,1 2 tendon and ligament issues,1 2 a pelvic prolapse and a tooth lost to resorption have also been reported.
Menstrual Shedding Data
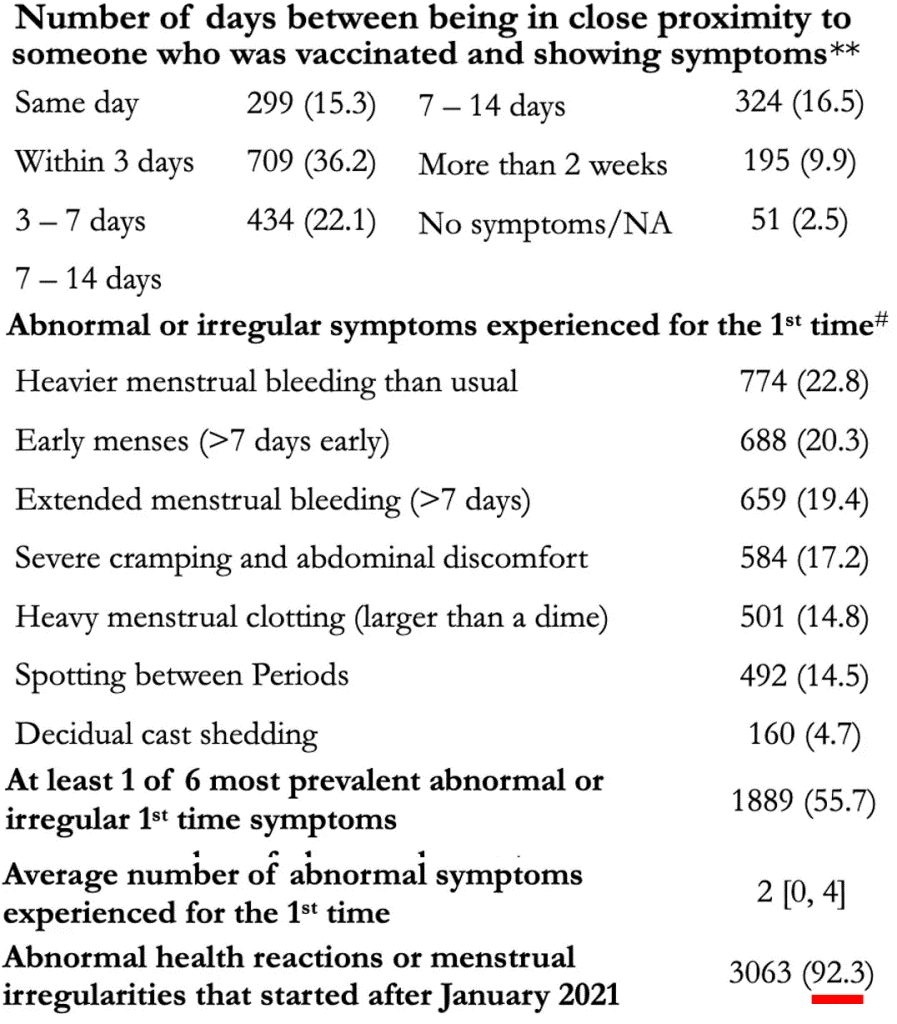
In addition to the reports compiled through virtual communication networks, MyCycleStory conducted an IRB approved study of 6049 female respondents (18 and older) which identified 3390 who had never had covid or a vaccine, and found 92.3% of them experienced menstrual abnormalities likely due to shedding which typically onset within 3 days of exposure:
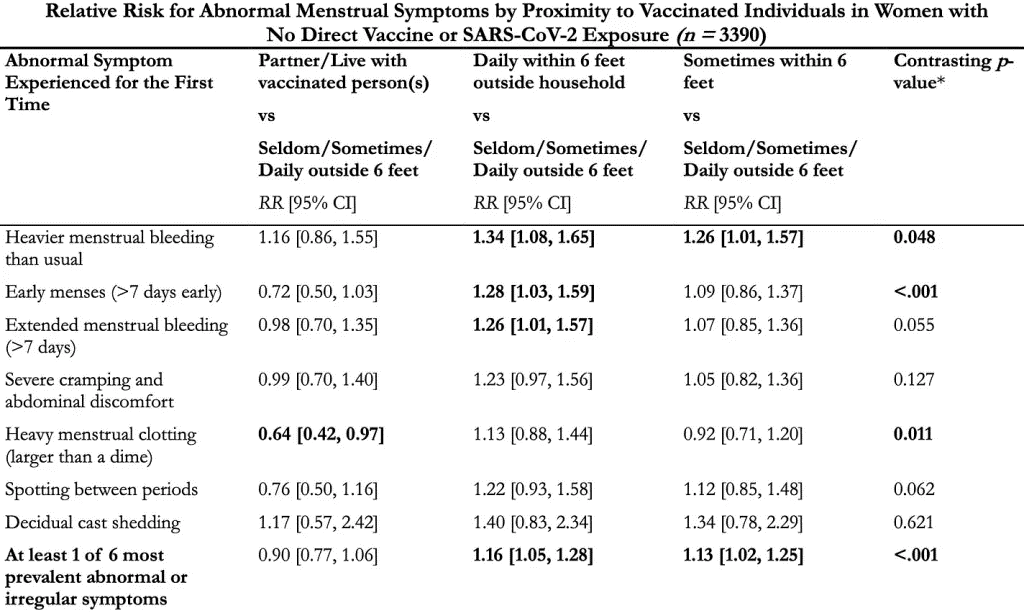
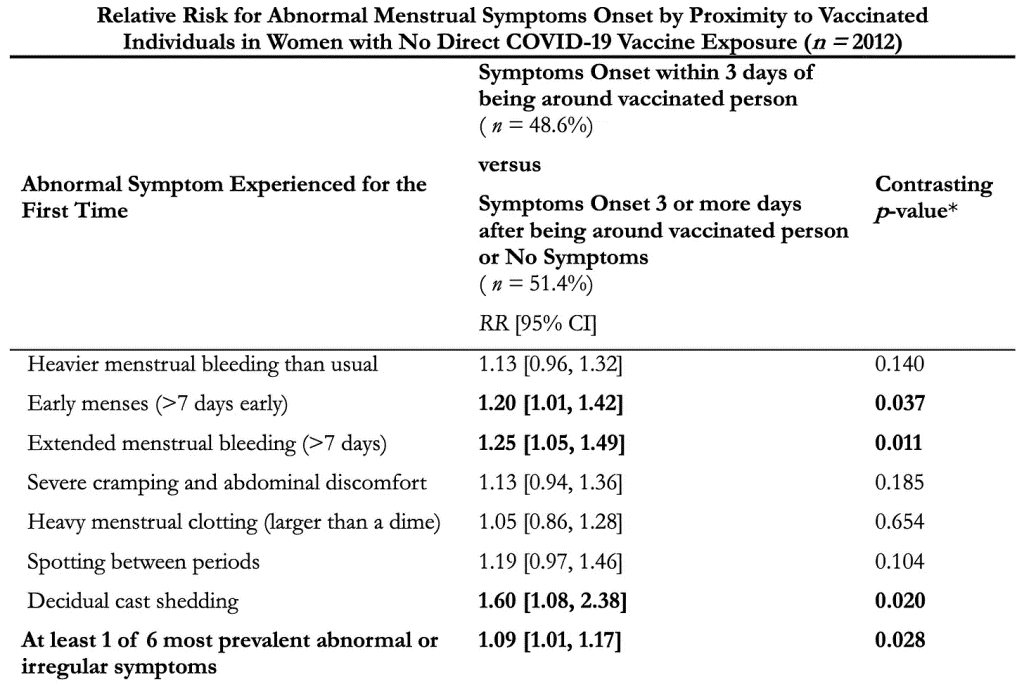
Additionally, they found these symptoms were strongly associated with shedding exposures:
Given how strong the associations are here (as almost everyone had these symptoms start after the covid vaccine roll-out) and how hard it is to conduct studies like this in the current political climate, I believe the case has been made (until data shows otherwise) that:
- The other common shedding symptoms detailed in this article would also show a similar strong association with being exposed to vaccinated people.
- Were a more sensitive study to be conducted, that many of the less frequent symptoms would be as well.
The Mechanistic Trap
A major problem with modern science is that different aspects (including those you see with your own eyes) are assumed to not exist unless an agreed upon mechanism exists to explain them. As such, I frequently will observe aspects (e.g., shedding) I can tell exist, but will be vociferously denounced by my peers for endorsing—despite the fact existing mechanisms are routinely disproved (e.g., depression is not a chemical imbalance) and new ones are regularly discovered.
Note: the mechanistic trap is often utilized to string together a series of misleading premises to assert a scientific orthodoxy (e.g., that the covid vaccines “do not persist in the body” or that “they cannot change your DNA”) rather than providing data to establish the assertion.
As such, a key focus has been on identifying mechanisms that could explain shedding.
Is Shedding Possible?
Typically, shedding occurs (e.g., from a live viral vaccine like MMR or polio) because a person “sheds” a self-replicating form of the disease. This results in a low concentration of the pathogen, which the shedder expels into their environment, then amplifies within the recipient and eventually reaches a comparable concentration to what was found in the “shedder.”
However, the mRNA vaccines do not contain self replicating pathogens, so limited options exist for what could spread, none of which make sense. For example:
- It’s possible some of the vaccine nanoparticles are excreted (especially when someone was recently vaccinated), but so few exist to begin with that it is unlikely that enough could ever be excreted to affect someone (let alone for an indefinite period), particularly since they cannot penetrate the skin, but many have reported reacting to touching surfaces shedders have contacted.
- If the spike protein produced by the vaccine is being shed, it seems nearly impossible that one’s tolerance to it could vary so greatly that one person could be asymptomatic from a large number of spike protein inside them, but another could become ill from the small amount that periodically exit that person and then are massively diluted in the environment.
At the same time however, Pfizer’s protocol for testing their vaccine:
- Prohibited pregnant women or those breast feeding from receiving the vaccine (or future doses if they had already received one).
- Stated it needed to be reported if a pregnant women (e.g., a healthcare worker in the trials) was exposed to the intervention by inhalation or skin contact from someone who had been vaccinated.
- Stated it needed to be reported if someone in the previous category (not vaccinated but exposed to someone who was) then was in close proximity to their wife and their wife was pregnant.
This suggested either that Pfizer knew shedding (and secondary shedding) was a real problem, or that they were following the existing standards—the FDA stipulates that gene therapies need to be evaluated for shedding before being given to humans (and furthermore be subsequently tested for shedding in humans). For context, both the FDA and the EMA (along with Moderna and Pfizer 1,2,3) classify the mRNA vaccines as a gene therapy.
Note: The first approved gene therapy, Luxturna, (which works like the J&J vaccine by using a modified virus to produce a target protein in the patient), is an eye medication (that costs $425,000.00 per eye) that treats a rare form of genetic vision loss (that DMSO also treats). Its prescribing information specifies that Luxturna can be found in a patient’s tears after injection. Hence, for the first seven days after injection, care needs to be taken to prevent anyone else from coming in contact with those tears and to prevent unintended shedding of the product. Another similar gene therapy, Roctavian was also found to shed (e.g., into semen), and the FDA advises those who receive it not to donate semen or impregnate someone for at least 6 months after administration. Finally, Zolgensma, a gene therapy, utilizing a different virus was also found to shed for a month, and its package insert advises that during this time, to be careful of how feces from the patients are disposed of (so no one else is exposed to it). Additionally, there is one other gene therapy on the market, but due to its design, shedding was unlikely (and hence undetected) so the FDA does not advise special precautions for its recipients. Curiously, the package inserts for all of the American covid vaccines do not mention shedding.
Shedding Mechanisms
At this point, I have identified three viable shedding mechanisms which can account for the existing data.
Exosome Mediated Shedding
Exosomes are small spheres continually released from cell membranes to communicate with their surroundings (many vital processes are regulated by exosomes) and transport intercellular contents. Mothers for example have exosomes in their breastmilk which make it through the digestive tract and deliver [micro]RNA to their developing babies which plays a critical epigenetic role in guiding their healthy development).
Note: exosomes are very similar to and inspired the creation of lipid nanoparticles (which were used to make the covid vaccines).
One of the unique aspects of covid-19 is that it “poisons” the exosome system.1,2,3,4,5
In turn, at the start of the pandemic, it was discovered that using therapeutic (healthy) exosomes produced dramatic results from severe covid-191,2,3 and numerous people I am close to almost certainly would have died had we not given them therapeutic exosomes.
Later, it was discovered that the covid vaccine also poisons the exosome system, which I believe is primarily due to the mRNA vaccine overproducing spike proteins which then get pushed out of the cells onto their membrane (at which point they bud off into spike protein studded exosomes). Additionally, those exosomes may also contain either vaccine mRNA or plasmids.
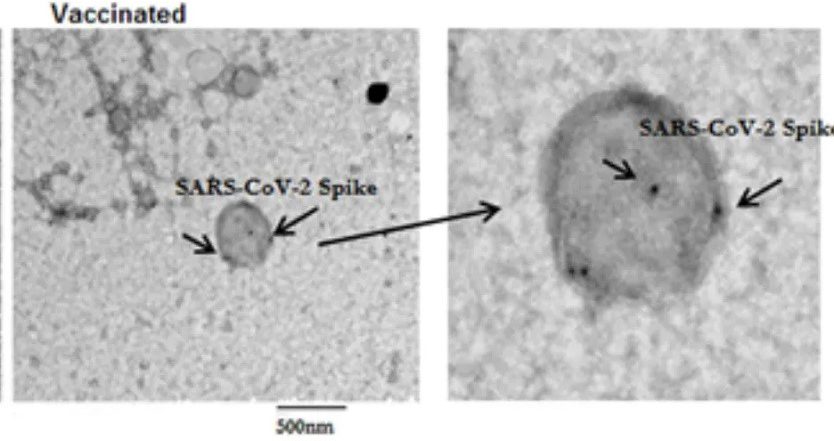
Note: The negative controls in the above experiment did have spike protein on their exosomes.
Presently, it has been shown that:
- Spike protein containing exosomes (which circulate in the bloodstream) spike after vaccination (and then decline) and appear to be one of the primary elements responsible for triggering the immune response that creates antibodies to the vaccine, as once spike protein coated exosomes are transferred to mice, the mice develop antibodies to the spike protein (along with increasing levels of various inflammatory cytokines).
- A 2023 peer-reviewed study found that unvaccinated children who were around covid-19 vaccinated parents developed an immune response to the spike protein that was not seen in children with unvaccinated parents—which meant something was indeed being shed. Additionally, they were also able to find spike protein antibodies in surgical masks worn by the physicians. This led the authors to hypothesize that antibodies were being directly transferred through the parent’s breath to their children.
- Significant amounts of (RNA containing) exosomes can be found in your breath, and those exosomes (which derive from the lungs) vary depending upon on the disease state someone has (“sicker” people have “worse” exosomes).1,2,3
Note: since this is a relatively new field of research, each paper is more sophisticated than the preceding one. - There was significant variation in how the covid vaccines were produced (e.g., that’s why there were “hot lots”), which caused some batches to concentrate in the lungs. In theory, this means that a portion of vaccine recipients could have briefly exhaled much of their vaccine (including the spike protein producing mRNA).
- The spike protein has a high (heparin dependent) affinity for binding to the surface of exosomes. So, if it was not already there when the exosome initially formed, it can also attach to exosomes traveling in the bloodstream.
- Long covid (and more severe acute covid) is characterized by the presence of spike protein studded exosomes (see this paper and this paper). Additionally, they also showed exosomes from covid patients are highly inflammatory (and potentially clot forming) and are taken up by the lung cells. The most detailed study (and imaging) of spike protein containing exosomes can be found in this paper (which also found that spike protein containing exosomes can circulate a year after covid infection).
Note: this study also found that covid triggers the production of spike protein-coated exosomes, and when lung cells are exposed to those exosomes, an immune response to the spike protein is triggered. - An inhaled vaccine was made from lung derived exosomes coated with spike proteins (they were lung derived so the lung cells would be more likely to absorb them). These spike protein exosomes both generated an immune response and were absorbed into the body. Once absorbed, those exosomes travel to other tissues and organs in the body, which (based on all the reports we’ve received and the patients we’ve seen) are known to be affected by shedding.
Collectively, this suggests that vaccinated people are continually exhaling spike protein studded exosomes, and that those around them are either inhaling them or touching surfaces they contacted, and then reacting either to the pathologic spike proteins on the exosomes (more likely), or taking up the exosome content and effectively being vaccinated with vaccine mRNA the exosomes traffic into their cells (less likely).
I find this theory compelling as it matches most of the available data, addresses the concentration issue (as what’s exhaled is comparable to what’s inhaled), and explains how a shedder can continuously produce the shedding agent (provided the vaccine mRNA persists). The major issue with it is that both exosomes and the spike protein have limited penetration through the skin (while no data exists on both together), so it is unclear if the allergic response alone that the spike protein generates could be sufficient to create the immediate reactions many have had to touching shedders.
Read the fourth part of the article
Author: A Midwestern Doctor
yogaesoteric
February 4, 2025